

Abstract
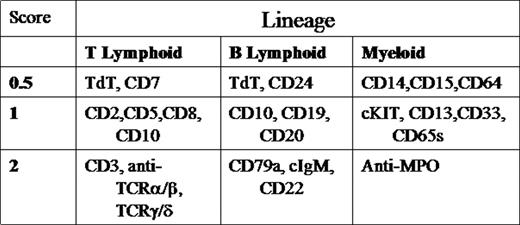
Current classification of childhood leukemia relies on morphologic, immunophenotypic, and molecular characteristics. aBL is rare and poorly understood. We retrospectively evaluated 7 patients diagnosed with aBL according to European Group for Immunological Classification of Leukemias (EGIL) criteria(2 or more lineages with a score greater than 2).
Among 269 leukemia patients diagnosed in 2001–2004, 7 (2.6%) were classified as having aBL. Clinical characteristics/course and laboratory data are listed below in Tables1&2.
CLINICAL CHARACTERISTICS & COURSE
| PATIENT | AGE | SEX | RACE | INITIAL WBC | TREATMENT | COURSE |
|---|---|---|---|---|---|---|
| 1 | 12 | F | AA | 5,600 | CCG1961-> CCG2891, HDARAC, HSCT | IND. FAILURE; R1:CNS,BM R2:BM R3:CNS,BM DOD, 24M |
| 2 | 17 | F | C | 81,600 | CCG2891 | R1:CNS,BM DOD, 10M |
| 3 | 2 | M | C | 40,000 | CCG1961 | RER; CR1, 16M |
| 4 | 2 | M | H | 5,630 | CCG1991-> CCG1961, HSCT | SER; CR1, 14M |
| 5 | 6 | F | H | 38,000 | CCG1961 | RER; CR1, 12M |
| 6 | 16 | M | AA | 150,000 | CCG1961-> AAML03P1 | IND. FAILURE; R1:BM DOD, 9M |
| 7 | 11 | M | C | 77,100 | AAML03P1, HSCT | RER; CR1, 7M |
| PATIENT | AGE | SEX | RACE | INITIAL WBC | TREATMENT | COURSE |
|---|---|---|---|---|---|---|
| 1 | 12 | F | AA | 5,600 | CCG1961-> CCG2891, HDARAC, HSCT | IND. FAILURE; R1:CNS,BM R2:BM R3:CNS,BM DOD, 24M |
| 2 | 17 | F | C | 81,600 | CCG2891 | R1:CNS,BM DOD, 10M |
| 3 | 2 | M | C | 40,000 | CCG1961 | RER; CR1, 16M |
| 4 | 2 | M | H | 5,630 | CCG1991-> CCG1961, HSCT | SER; CR1, 14M |
| 5 | 6 | F | H | 38,000 | CCG1961 | RER; CR1, 12M |
| 6 | 16 | M | AA | 150,000 | CCG1961-> AAML03P1 | IND. FAILURE; R1:BM DOD, 9M |
| 7 | 11 | M | C | 77,100 | AAML03P1, HSCT | RER; CR1, 7M |
MORPHOLOGY, IMMUNOPHENOTYPE & CYTOGENETICS
| PATIENT | FAB MORPHOLOGY | FLOW CYTOMETRY | EGIL SCORE(T/B/M) | CYTOGENETICS/FISH |
|---|---|---|---|---|
| * =Peripheral Blood | ||||
| 1* | L1, M5 | CD3, CD7, pCD5, CD33,MPO | 3.5/0/3 | 6,XX,add(1)(p22);t(3;12)(p24;p13),del(6)(q21q22),del(8)(p21),-9,del(13)(q13q14), +22 |
| 2* | L1, M2 | P1: CD19, CD22, CD33, Tdt P2: CD2,CD14,CD15, CD33, MPO | 2/3.5/4 | 46,XX,der(8)t(8;?;17)(q11.2;?;q21),der(9)t(8;9)(q21.2;p12),del(15)q21), der(17)t(15;?;17)(q21;?;q11.2) |
| 3 | L2 | P1: CD33, CD34 P2: CD13, CD15, CD10, CD19, CD22 | 0/4/2.5 | 46, XY, del12p-/TEL deletion |
| 4 | L1 | CD19,CD22, CD13, CD15, CD33 | 0/3/2.5 | 46, XY |
| 5 | L1, M5 | CD19, pCD20, CD22, CD13, CD15, pCD33 | 3.5/0/3.5 | 46, XY, del(5)(q15q33), dic(7;9)(p11.2;p12),inv(9)c,t(10,11)(p13;q21) |
| 6 | L2 | cCD3, pCD5, CD7, CD13, CD15, CD33,pCD117 | 0/4/3.5 | 46, XX/Trisomy 10 |
| 7* | L1, M5 | CD2,CD3,CD7, TdT, pCD22,CD13, CD15, pMPO, CD117 | 4/1/4.5 | 46, XY |
| PATIENT | FAB MORPHOLOGY | FLOW CYTOMETRY | EGIL SCORE(T/B/M) | CYTOGENETICS/FISH |
|---|---|---|---|---|
| * =Peripheral Blood | ||||
| 1* | L1, M5 | CD3, CD7, pCD5, CD33,MPO | 3.5/0/3 | 6,XX,add(1)(p22);t(3;12)(p24;p13),del(6)(q21q22),del(8)(p21),-9,del(13)(q13q14), +22 |
| 2* | L1, M2 | P1: CD19, CD22, CD33, Tdt P2: CD2,CD14,CD15, CD33, MPO | 2/3.5/4 | 46,XX,der(8)t(8;?;17)(q11.2;?;q21),der(9)t(8;9)(q21.2;p12),del(15)q21), der(17)t(15;?;17)(q21;?;q11.2) |
| 3 | L2 | P1: CD33, CD34 P2: CD13, CD15, CD10, CD19, CD22 | 0/4/2.5 | 46, XY, del12p-/TEL deletion |
| 4 | L1 | CD19,CD22, CD13, CD15, CD33 | 0/3/2.5 | 46, XY |
| 5 | L1, M5 | CD19, pCD20, CD22, CD13, CD15, pCD33 | 3.5/0/3.5 | 46, XY, del(5)(q15q33), dic(7;9)(p11.2;p12),inv(9)c,t(10,11)(p13;q21) |
| 6 | L2 | cCD3, pCD5, CD7, CD13, CD15, CD33,pCD117 | 0/4/3.5 | 46, XX/Trisomy 10 |
| 7* | L1, M5 | CD2,CD3,CD7, TdT, pCD22,CD13, CD15, pMPO, CD117 | 4/1/4.5 | 46, XY |
5 patients had abnormal karyotypes and/or FISH studies; none had MLL rearrangements or t(9;22). Induction treatment consisted of AML-type therapy (CCG 2891 /COG AAML03P1) in 2 patients who achieved CR by day 28. Two patients received ALL-type therapy (CCG 1961) and entered CR by Day 28. Three patients required dose intensification due to induction failure: 2 switched from ALL to AML-type therapy. Post induction chemotherapy was given in 4 cases; allogeneic HSCT in 3 cases (2 in CR1; 1 in 2nd relapse). 2/4 and 2/3, respectively, remain alive in 1st CR after chemotherapy or HSCT. All 3 deaths were from relapse of aBL within 2 yrs from diagnosis & occured in adolescents with complex karyotypes. In our experience, pediatric aBL represents a high risk population, especially in adolescents. Intensive induction chemotherapy is necessary in the majority of cases to achieve CR, although it is unclear whether ALL or AML-type therapy is superior. MLL & t(9;22) may not be as common in pediatric aBL as previously described. Collaborative trials and biologic studies are clearly needed for better understanding and outcomes.

