

Abstract
Abstract 1909
Poster Board I-932
The International Prognostic Scoring System (IPSS) for primary myelofibrosis (PMF) utilizes five independent predictors of inferior survival; of these, a hemoglobin level <10 g/dL has the highest impact on survival (Cervantes et al. Blood 2009;113:2895). In the current study, we examined the additional prognostic impact of transfusion need at diagnosis or becoming transfusion-dependent in the first year of diagnosis. These events were also correlated with JAK2 or TET2 mutational status.
Patients were selected from the Mayo Clinic PMF database based on availability of bone marrow histology and IPSS-relevant information at diagnosis and follow-up transfusion history at one year from diagnosis. WHO criteria were used for PMF diagnosis. Patients who underwent allogeneic hematopoietic cell transplantation were censored at time of transplant. Patient records were updated in July, 2009. Survival curves were constructed using the Kaplan-Meier method and compared by the log-rank test. Multivariable survival was analysed using Cox regression model.
A consecutive cohort of 254 patients was studied (median age 59 years; range 28-87; 159 males). IPSS risk category was low, intermediate (int)-1, int-2 and high in 75, 71, 62 and 46 patients, respectively. JAK2V617F was present in 118 (62%) of 192 patients and TET2 mutations in 6 (13%) of 45 patients evaluated. Transfusion need at diagnosis was documented in 62 patients whereas an additional 22 patients became transfusion-dependent during the first year of their diagnosis. The remaining 170 patients remained transfusion-independent for at least one year post-diagnosis.
To date, 139 patients have died. In patients who are alive, median follow-up was 5.3 years. Median survivals in IPSS high, Int-2, Int-1 and low risk patients were, 3, 3.9, 6.8 and 12.8 years, respectively (p<0.0001). Median survival for patients requiring transfusions at diagnosis was similar to that of patients who became transfusion-dependent in their first year of diagnosis, and both were significantly shorter than the median survival seen in patients who remained transfusion-free during the first year post-diagnosis: 2.9, 2.2 and 9.7 years, respectively (p<0.0001; figure). Multivariable analysis confirmed the IPSS-independent prognostic value of transfusion status-based risk stratification. Neither JAK2 nor TET2 mutational status correlated with transfusion need.
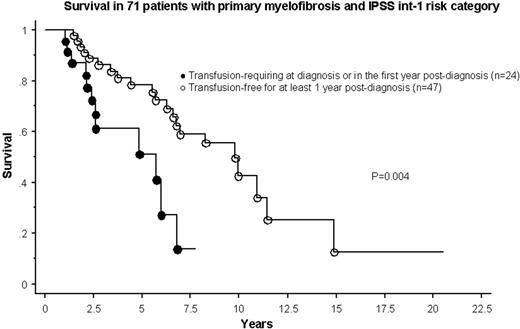
In PMF, becoming transfusion-dependent in the first year of diagnosis is prognostically as detrimental as requiring transfusions at initial presentation. These events are not affected by JAK2 or TET2 mutational status and confer an IPSS-independent adverse prognosis. The ability to identify Int-1 risk patients with shortened survival (Figure) holds major treatment implications. 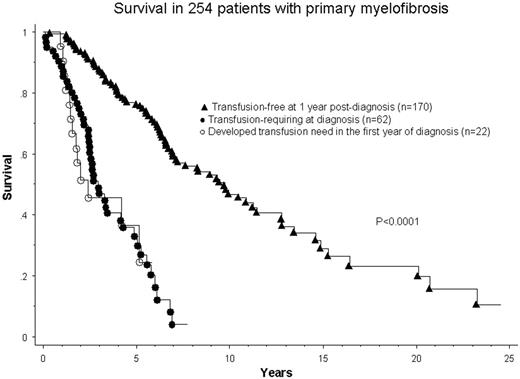
No relevant conflicts of interest to declare.

