

Abstract
Abstract 2315
Multiple lines of evidence have demonstrated a relationship between high on-treatment platelet reactivity (HPR) measured by multiple platelet assays and adverse clinical ischemic events. Although the Working Group on High On-Treatment Platelet Reactivity recently provided a consensus opinion on the definition of HPR, correlations between HPR cut-offs have not been validated yet. Therefore, we performed this study to provide a comprehensive analysis on the agreement and correlation of HPR cut-offs based on the consensual definition among the different platelet function measurements.
We analyzed data from coronary intervention-treated patients on dual antiplatelet therapy (n = 962). Platelet measures were concurrently 5 and 20 μM ADP-stimulated light transmittance aggregometry (LTA), the VerifyNow P2Y12 analyzer, and flow cytometric analysis of vasodilator-stimulated phosphoprotein (VASP)-platelet reactivity index (PRI). As the Working Group noted, HPR cut-offs were defined as 5 and 20 μM ADP-induced maximal platelet aggregation (PRmax) > 46% and 59%, the VerifyNow P2Y12 assay > 240 P2Y12 reaction unit (PRU), and the VASP-PRI > 50%, respectively. Agreement between the consensual cut-off points of different tests was determined by kappa statistics, and 95% confidence intervals (CI) were also calculated. Receiver-operating characteristics (ROC) curve analysis was performed to identify the matched points for consensual definition-based cut-offs for HPR.
The consensual cut-off as 5μmol/l ADP-induced PRmax >46% showed a substantial agreement with 20 μmol/l ADP-induced PRmax, however, this cut-off showed a moderate agreement with the VerifyNow P2Y12 assay > 240 PRU and the VASP-PRI > 50%, respectively (Table 1). Fair correlations were observed between ADP-induced PRmax, the VerifyNow P2Y12 assay, and VASP-PRI according to the ROC curve analyses (Table 2). The cut-offs for 5μmol/l ADP-induced PRmax >46% based HPR matched well with the VerifyNow P2Y12 assay > 284 PRU (AUC 0.791, 95% CI 0.763–0.819, sensitivity 62.0%, and specificity 80.7%, p < 0.001), and the VASP-PRI > 60.3% (AUC 0.788, 95% CI 0.759–0.816, sensitivity 78.2%, and specificity 70.2%, p < 0.001) by the ROC curve analysis, respectively. The consensus-defined cut-offs of VerifyNow P2Y12 assay and VASP index overestimated HPR risk based on LTA cut-offs.
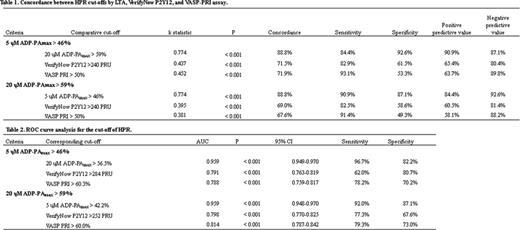
Although the VerifyNow P2Y12 and VASP assay correlated significantly with LTA, there are moderate agreements and fair correlations among the consensual cut-offs of HPR. These data suggest the platelet function measurements need to be improved to become clinically used diagnostic tests and the need for a new cut-offs to balance safety and efficacy of P2Y12 receptor antagonists. Further, it still may be too early to define the gold standard method for assessing platelet reactivity and generally acceptable cut-off values.
No relevant conflicts of interest to declare.

