

Abstract
Follicular lymphoma grade 3 (FLG3) are recognized as a distinct entity in the World Health Organization classification of lymphoma. FLG3 are defined as > 15 centroblasts per high power field and are further subdivided into A or B on the basis of the presence of centrocytes. Their natural history is similar to that of diffuse large B cell lymphomas (DLBCL) and there is still debate about their optimal management.
We conducted a retroprospective analysis of 156 patients with FLG3 receiving frontline treatment at MD Anderson Cancer Center between 06/1973 and 11/2004. Multivariate analysis (MVA) was performed using Hazard Ratio (HR) Cox regression with backward stepwise selection. Logistic regression with odds ratio (OR) was used for MVA of categorical variable.
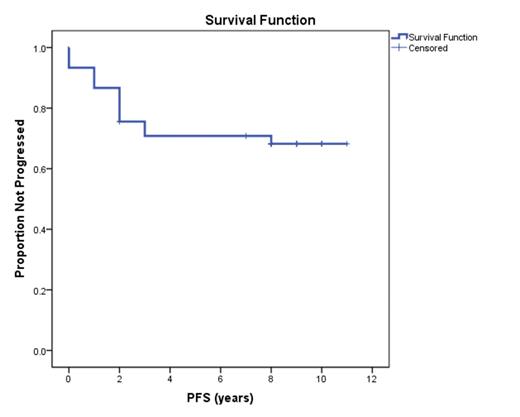
Patient baseline characteristics are shown in the Table. Forty-five (29%) patients received R-CHOP, of which 12 (27%) received more than 6 cycles and 9 (20%) and radiation therapy as consolidation. In particular, patients with stage I/II disease (9) all received 5-6 cycles, with additional radiation therapy consolidation in 4 patients. The overall response rate was 100% and 43 (96%) patients achieved complete remission (CR). After a median follow-up of 9 (2-12) years, median PFS has not been reached with 14 (31%) patients relapsing. Nearly all relapses occurred within 3 years, except for 1 patient who relapsed after 8 years and achieved a second durable CR with single agent Rituximab (Figure). On MVA, the only characteristic associated with a shorter PFS was the presence of > 4 nodal sites (HR 4.2, p=0.03). Among relapsed patients, 3 (21%) transformed to DLBCL (1 at first relapse) and died. Six (43%) relapsed patients received stem cell transplant (1 allogeneic) and 5 (36%) received more than 2 salvage regimens. Median OS has not been reached for all R-CHOP treated and relapsed patients. On univariate analysis, the only factor associated with a shorter OS after relapse was transformation (p=0.01). Baseline characteristics associated with transformation on MVA were IPI score 3-4 (OR 1.1, p=0.004) and elevated LDH (OR 2.4, p=0.01). Nine patients died, 2 (22%) of lymphoma progression, 4 (44%) of therapy-related acute myeloid leukemia (AML) and 3 (32%) of cancer-unrelated causes On MVA, factors associated with shorter OS after R-CHOP were age > 60 years (HR 11, p=0.02) and LDH > 618 IU/L (HR 5.9, p=0.01). On univariate analysis, age > 60 years was the only factor associated with AML onset (p=0.04).
| PATIENTS CHARACTERISTICS (N=45) | NUMBER (%) |
|---|---|
| AGE ≥ 60 years | 21 (47) |
| MALES | 23 (51) |
| ECOG 1-2 | 1 (2) |
| HISTOLOGY 3B | 40 (89) |
| STAGE 3-4 | 36 (80) |
| NODAL SITES > 4 | 17 (38) |
| BULKY DISEASE (> 6 cm) | 5 (11) |
| EXTRANODAL SITES > 1 | 6 (13) |
| BONE MARROW INVOLVEMENT | 14 (31) |
| B SYMPTOMS | 5 (11) |
| IPI 3-4 | 8 (18) |
| FLIPI 3-5 | 15 (33) |
| HEMOGLOBIN < 12 g/dL | 8 (18) |
| LDH > 618 IU/L | 11 (24) |
| BETA-2-MICROGLOBULIN > 4 mg/L | 8 (18) |
| PATIENTS CHARACTERISTICS (N=45) | NUMBER (%) |
|---|---|
| AGE ≥ 60 years | 21 (47) |
| MALES | 23 (51) |
| ECOG 1-2 | 1 (2) |
| HISTOLOGY 3B | 40 (89) |
| STAGE 3-4 | 36 (80) |
| NODAL SITES > 4 | 17 (38) |
| BULKY DISEASE (> 6 cm) | 5 (11) |
| EXTRANODAL SITES > 1 | 6 (13) |
| BONE MARROW INVOLVEMENT | 14 (31) |
| B SYMPTOMS | 5 (11) |
| IPI 3-4 | 8 (18) |
| FLIPI 3-5 | 15 (33) |
| HEMOGLOBIN < 12 g/dL | 8 (18) |
| LDH > 618 IU/L | 11 (24) |
| BETA-2-MICROGLOBULIN > 4 mg/L | 8 (18) |
R-CHOP is an effective treatment for patients with FLG3 and small number of nodal sites, with rare late progressions. The incidence of transformation is low but is fatal. Onset of second myeloid malignancies is the main cause of death and warrants caution in elderly patients.
No relevant conflicts of interest to declare.

