

Abstract
Introduction: The only curative treatment approach for patients with Chronic Myelomonocytic Leukemia (CMML) is allogeneic hematopoietic stem cell transplantation (HSCT), but disease relapse after transplantation is a major concern. Predictors for disease outcome after HSCT are limited. However, unfavorable cytogenetic abnormalities have been shown to serve as predictors for relapse after transplantation. The aim of this large multicentric, international study was to retrospectively determine the impact of cytogenetic information according to the CMML-specific prognostic scoring system (CPSS) on outcome after allogeneic HSCT.
Patients and Methods: Patients were selected from the EBMT database who had received a first allogeneic HSCT for the treatment of CMML between 2000 and 2015. 268 centers participated into this study. In total, 1503 patients were included. Impact of CPSS-cytogenetic classification was analyzed regarding overall survival (OS) and cumulative incidence of relapse and non-relapse mortality after HSCT (gray test).
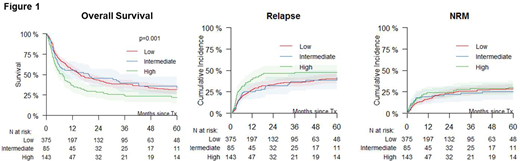
Results: 488 female (32.5%) and 1013 male (67.5%) patients were included to the study. Median age at HSCT was 57.6 years (range 0.3-75.4). At time of HSCT, only 422 (28.1%) patients were in complete remission, whereas 1004 (66.8%) had active disease (77 missing). Matched related donor HSCT was performed in 35.7% of the patients, matched unrelated donor HSCT in 57.6%, mismatched related in 3.3% and mismatched unrelated in 3.4%. Bone marrow (12.6%), peripheral blood (84.3%), or both (0.3%) served as the stem cell graft. Cord blood was used as a graft in 2.8%. Myeloablative preparative regimens wereused in 223 patients (15.0%), and less intensive regimens were given to 1268 patients (85.0%). Median survival of patients included into this study was 52.2 months. 637 patients had sufficient cytogenetic information according to CPSS (866 missing), complete relapse information was available in 1385 patients. 143 patients could be categorized into CPSS-high, 85 in intermediate and 375 in low risk cytogenetics, respectively. In univariate analysis high risk CPSS cytogenetic information was found to be strongly associated with OS (low 38% (32-44%), intermediate 41% (30-53%), high 26% (18-34%)), and higher cumulative incidence of relapse (low 40% (35-46%), intermediate 42% (30-54%), high 48% (39-56%)), but not with non relapse mortality (low 28% (23-33%), intermediate 25% (16-35%), high 30% (22-38%)) at 60 months (Figure 1).
Conclusion: In this international, multicentric analysis we show that CMML patients with high-risk cytogenetics had significantly worse OS after HSCT than patients with intermediate or low risk cytogenetics according to CPSS. New therapeutic strategies to prevent relapse after HSCT in CMML patients with high-risk cytogenetics are needed.
Koenecke:Amgen: Consultancy; abbvie: Consultancy; BMS: Consultancy; Roche: Consultancy. Beelen:Medac: Consultancy, Other: Travel Support. Finke:Novartis: Consultancy, Honoraria, Other: travel grants, Research Funding; Riemser: Consultancy, Honoraria, Research Funding; Medac: Consultancy, Honoraria, Other: travel grants, Research Funding; Neovii: Consultancy, Honoraria, Other: travel grants, Research Funding. Niederwieser:Novartis: Research Funding; Miltenyi: Speakers Bureau. Chalandon:Roche: Membership on an entity's Board of Directors or advisory committees, Other: Travel costs. Ganser:Novartis: Membership on an entity's Board of Directors or advisory committees. Kobbe:Amgen: Honoraria, Research Funding; Roche: Honoraria, Research Funding; Celgene: Honoraria, Other: Travel Support, Research Funding.

