

Introduction: Early immune reconstitution without severe graft-versus-host disease (GVHD) is required for the success of allogeneic hematopoietic stem cell transplantation (allo-HSCT). We showed that MEK inhibitors suppress GVHD but retain antiviral immunity and graft-versus-tumor (GVT) effects (Shindo, Blood2013; Itamura, Shindo, JCI Insight2016). Furthermore, we have shown that they attenuate graft rejection but spare thymic function following rat lung transplantation (Takahagi, Shindo, Am J Respir Cell Mol Biol2019). Here we analyzed their effects on human polyclonal T cell reconstitution in xenogeneic transplant by evaluating T-cell receptor (TCR) repertoire diversity.
Methods: As a xenogeneic GVHD model, human PBMCs were infused to NOD/Scid/JAK3null mice, immunodeficient mice lacking T/B/NK cells, after total body irradiation. Vehicle, tacrolimus, or the MEK inhibitor trametinib was administered from day 0 through 28 or day 15 through 28. Human TCR repertoire diversity was evaluated by an adapter ligation PCR method with next generation sequencing (Shindo, Oncoimmunol2018) in the liver, lung, and spleen. The assignment and frequencies of TCRαV/J clones were determined at the single-cell level. Their diversity and clonality were evaluated by Inv. Simpson's index 1/λ.
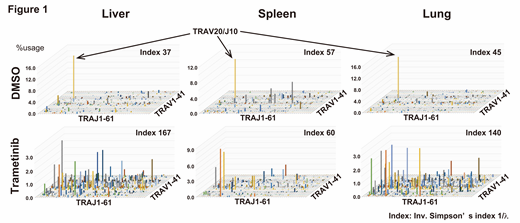
Results: Trametinib prolonged their survival compared with vehicle (median survival: 88 vs 46 days, p<0.05). It enhanced engraftment of human leukocytes in peripheral blood (human CD45+cells: 11.0 vs 2.5%), but prevented their infiltration into the lung (human CD45+cells on day 60: 1.5 vs 6.5%). Treatment with vehicle resulted in skewed TCR repertoire with limited clones in the spleen, liver and lung. Interestingly, expansion of one specific clone (TRAV20/J10) was commonly observed, which might reflect the GVHD-inducing pathological clone (Fig. 1: 3D graphs show the frequencies of TCRαV/J clones). However, trametinib enabled diverse and polyclonal T cell engraftment without the TRAV20/J10 clone. While CD4+and CD8+T cells within injected human PBMCs mainly consisted of naïve (CD45RA+CD27+) and central memory (CD45RA-CD27+) T cells, infiltrating T cells in each organ showed effector memory (CD45RA-CD27-) T cell phenotype. Of note, CD8+T cells in the bone marrow, spleen, and lung of trametinib-treated recipients showed reduced effector memory T cells (CD45RA-CD27-) compared with vehicle-treated mice at day 28 (bone marrow 21.7 vs 74.7%, p<0.01; spleen 66.3 vs 88.7%, p<0.05; lung 33.0 vs 72.5%, p<0.05), which indicating that MEK inhibition suppresses functional differentiation of human T cells in vivo. Furthermore, trametinib treatment from day 14 to 28 still ameliorated clinical GVHD score, and maintained polyclonal T cell repertoire.
Conclusions:GVHD can be characterized with skewed TCR repertoire diversity and expansion of pathological T cell clones in the target tissues. Trametinib suppresses GVHD but maintains polyclonal T cell reconstitution, even in established GVHD. These results explain the facts that MEK inhibitors separate GVHD from GVT effects/antimicrobial immunity. Furthermore, MEK inhibition enhances immune reconstitution after allo-HSCT, which would avoid post-transplant complications.
Shindo:Novartis: Research Funding. Kitaura:Repertoire Genesis Inc.: Employment. Okada:Bristol-Myers Squibb: Research Funding; Japan Agency for Medical Research and Development: Research Funding. Shin-I:BITS Co., Ltd: Equity Ownership. Suzuki:Repertoire Genesis Inc.: Equity Ownership. Takaori-Kondo:Celgene: Honoraria, Research Funding; Novartis: Honoraria; Bristol-Myers Squibb: Honoraria, Research Funding; Ono: Research Funding; Takeda: Research Funding; Kyowa Kirin: Research Funding; Chugai: Research Funding; Janssen: Honoraria; Pfizer: Honoraria. Kimura:Ohara Pharmaceutical Co.: Research Funding; Novartis: Honoraria, Research Funding.

