

Background: Acute graft-versus-host disease (aGVHD) post allogeneic hematopoietic stem cell transplantation (HCT) has a significant impact on morbidity and mortality. The standard first-line therapy for grade II-IV aGVHD is systemic corticosteroids (CS), which provide effective control in 40%-60% of patients. Patients may be unable to taper steroids due to new organ involvement or aGVHD flares. The objective of this retrospective multicenter study was to describe the clinical course, outcomes, and hospital readmissions for patients with aGVHD who were refractory to or dependent on systemic CS.
Methods: A multicenter retrospective chart review was conducted at 11 large US academic and community transplant centers to identify patients who had their first HCT between Jan 1, 2014, and June 30, 2016, and subsequently developed grade II-IV aGVHD (defined by International Bone Marrow Transplant Registry Severity Index). Patients who participated in a GVHD prophylaxis trial or used Janus kinase inhibitors were excluded. Steroid dependence (SD)/steroid refractory (SR) was defined as the use of additional systemic anti-GVHD therapy, inability to taper high-dose steroids (≥1 mg/kg) by ≥25%, or tapering of CS dose by ≥25% but not <10 mg/day. Clinical outcomes included changes in aGVHD grade or organs involved, aGVHD reoccurrence, and all-cause mortality.
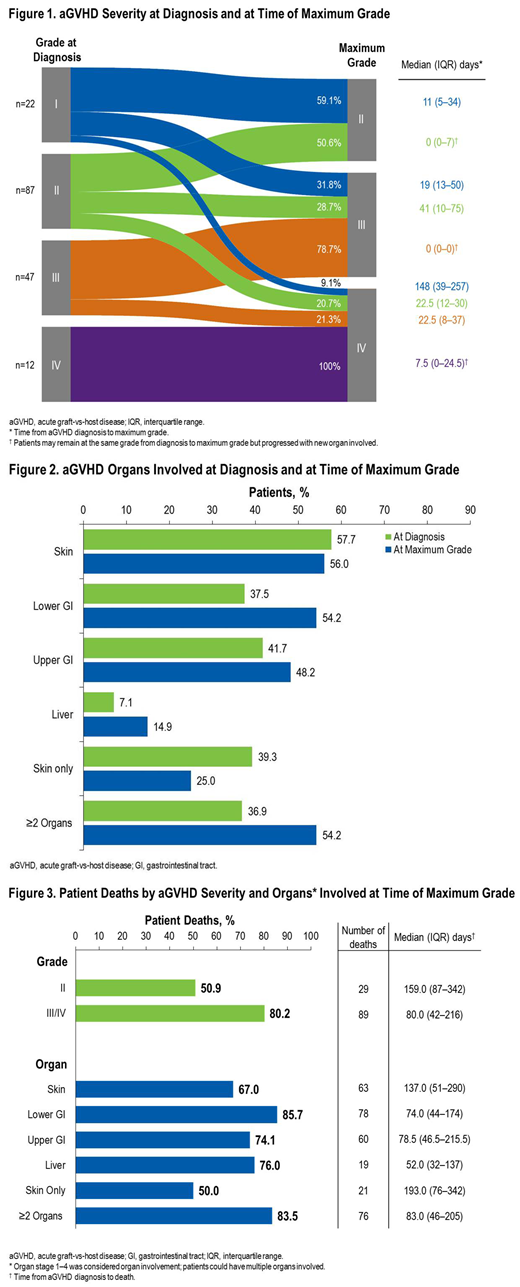
Results: Patient (N=168) mean age was 55 years, and 64% were male. The stem cell source was peripheral blood for 74% of patients. Median time from transplant to aGVHD diagnosis was 30 days (interquartile range [IQR]: 21-49). At the time of aGVHD diagnosis, most patients had grade I or II (65%; Figure 1) disease: 39% had skin involvement only; 38% had lower gastrointestinal (GI) involvement; and 37% had ≥2 organs involved (Figure 2). At the time of maximum aGVHD grade, most patients (66%) had grade III-IV disease: 25% had skin involvement only; 54% of patients had lower GI involvement; and 54% had ≥2 organs involved. Between the time of diagnosis and maximum aGVHD grade, 54% of patients had new organ involvement or an increase in aGVHD grade. Median time from diagnosis to maximum grade was 6.0 days.
Of the 146 patients with grade II-IV aGVHD at diagnosis, 82% (119/146) were given systemic CS as first-line therapy, and 49% (72/146) initiated systemic CS on the day of diagnosis. Among the 119 patients, the average starting daily dose was 77 mg (0.9 mg/kg) for prednisone and 166 mg (1.8 mg/kg) for methylprednisolone. During follow-up (median 194 days from aGVHD diagnosis to death/last visit, IQR: 58-720), 36% of patients had an increase in steroid dose, and 88% were unable to taper below 10 mg/day. aGVHD recurred in 42% of patients (70/168) and was managed by increasing the CS dose in 79% of these patients. Over half of patients (53%; 89/168) received additional systemic anti-GVHD therapy; of those, 41% had an increase in CS dose before receiving additional therapy. Median time from CS initiation to additional therapy was 21 days. Frequently used additional therapies included sirolimus (19%), polyclonal antibodies (antithymocyte globulin/antilymphocyte globulin; 18%), mycophenolate mofetil (17%), tocilizumab (16%), extracorporeal photopheresis, and etanercept (both 13%). 26% (23/89) used ≥2 additional therapies.
Overall, 57% of patients (95/168) required hospital readmission(s); 24% had ≥2 readmissions within 100 days post-HCT, with a mean inpatient length of stay of 50 days. Half (51%) of patients experienced an infection within the first 100 days post-HCT. Relapse of the underlying malignancy was reported in 35 patients (21%). Overall, 70% of patients (118/168) died at a median of 118 days (IQR: 62.0-234.1) from aGVHD diagnosis; 82% of patients with aGVHD progression died at a median of 116.0 days (IQR: 49-223), and 80% of patients with maximum grade III-IV aGVHD died at a median of 80 days (IQR: 42-216). Additionally, 86% of patients with lower GI aGVHD died at a median of 74.0 days (IQR: 44-174) (Figure 3).
Conclusions: The majority of patients with aGVHD had severe and rapidly progressing disease. These findings indicate that clinical outcomes were poor among patients with SR and SD, with a mortality rate of 70% within 4 months of aGVHD diagnosis. Most patients required hospital readmission with an extended length of stay. The rapidly worsening clinical course further emphasizes the need for effective and tolerable therapies that prevent or reverse disease progression.
Yu:Incyte: Employment, Equity Ownership. Hanna:Asclepius Analytics: Employment. Paranagama:Incyte: Employment, Equity Ownership. Tang:Asclepius Analytics: Employment. Naim:Incyte: Employment, Equity Ownership. Galvin:Incyte: Consultancy.

