

Introduction
Painful vaso-occlusive crisis (VOC) is a hallmark of sickle cell disease (SCD). When the pain cannot be managed with home analgesics, patients often present to the Emergency Department (ED) in order to obtain relief. In the ED, the patient may encounter barriers to care that include provider bias, prolonged time to initial analgesic, and inadequate opioid dosing. The goal of this retrospective, single-institution study was to evaluate whether there was an association between the time to initial analgesic and the rate of admission for patients with SCD presenting with VOC.
Methods
A retrospective, single-institution chart review of adult ED visits between January 29, 2019 and June 30, 2019 was conducted for patients with a history of SCD who presented to the Adult ED for pain related to a VOC. Patients were divided into two cohorts: patients with a calculated door-to-dose time of ≤ 2 hours and patients with a door-to-dose time of > 2 hours. Registration time, time of first opioid administration, and disposition decision were recorded for each visit. The primary outcome of interest was to compare the rate of admission between the two cohorts.
Results
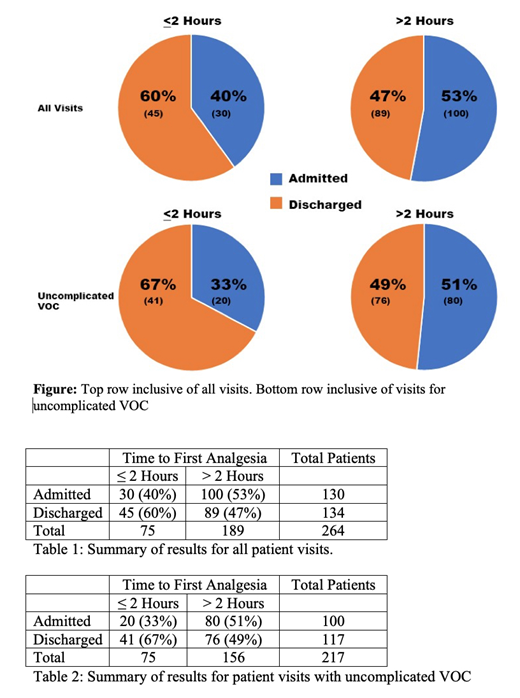
During the study period, 43 unique patients met the inclusion criteria. These patients were seen for a total of 264 visits for VOC-related acute pain. The overall rate of admission was 49% (130 of 264). The cohort of patients receiving analgesia within 2 hours included 75 (28% of total) subjects, whereas 189 (72%) patients received their first analgesic dose after 2 hours. The admission rate for patients with a door-to-dose time ≤ 2 hours was not significantly different from that for patients with a door-to-dose time > 2 hours (40% vs 53%, P = 0.076)
A subgroup analysis was performed on patients presenting to the ED with uncomplicated VOC. This analysis excluded any visits in which patients presented for pain with additional complications (e.g. fever, chest pain, nausea/vomiting, shortness of breath). The purpose of this exclusion was to control for possible confounding by severity or complexity of illness, given that patients who have higher acuity are more likely to be seen faster, but also more likely to be admitted. A total of 47 patient visits from 23 unique patients were excluded from the total visits to perform the subgroup analysis. The most prevalent reasons for exclusion included URI (n=7), nausea and vomiting (n=7), shortness of breath (n=7), and fever (n=7). A subgroup of 37 patients was seen for a total of 217 visits for uncomplicated, VOC-related acute pain. The overall rate of admission was 46% (100 of 217). In 61 (28%) of the encounters analgesia was administered within 2 hours of registration, whereas in 156 (72%) of the encounters the first analgesic was received after 2 hours. In this subgroup of patients presenting with uncomplicated VOC, the admission rate for patients with a door-to-dose time ≤2 hours was significantly lower than that for patients with a door-to-dose time > 2 hours (33% vs 51%, P = 0.016).
Conclusion
For the entire cohort of patients with sickle cell disease, the administration of analgesia within 2 hours did not result in a statistically significant decrease in rate of admission. In the subgroup analysis, which excludes VOC-related pain visits with complications, the administration of analgesia within 2 hours did result in a statistically significant decrease in the rate of admission. This demonstrates the association between rapid administration of analgesia and a greater likelihood of discharge in the setting of uncomplicated VOC. Based on these preliminary findings, it would be reasonable to allocate additional resources to ensure the rapid administration of analgesia in patients with uncomplicated acute VOC pain crises.
Dupont:Pfizer: Other: Grant Support. Baer:Al Therapeutics: Research Funding; Incyte: Research Funding; Abbvie: Research Funding; Takeda: Research Funding; Kite: Research Funding; Forma: Research Funding; Astellas: Research Funding. Wilkerson:Pfizer: Other: Grant, Research Funding; Roche: Research Funding; Coaptech: Research Funding; Provay Pharmaceuticals: Research Funding; Cepheid: Other: Research Equipment; Janssen: Research Funding.

