

Introduction:
Sickle cell disease (SCD) is characterized by hemolytic anemia and vaso-occlusive episodes associated with multi-organ dysfunction. Chronic kidney disease is a common complication and associated with increased mortality. Opioid analgesics are used in SCD patients for pain relief, often starting at a young age and continuing through adulthood. In SCD mouse models, chronic opioid exposure worsens nephropathy leading to increased glomerular mesangial volume and fractional kidney mass as well as albuminuria. We evaluated the association of opioid analgesic use and albuminuria in adult patients with sickle cell disease.
Methods:
We conducted a cross-sectional study of patients with sickle cell anemia (HbSS and HbSβ0thalassemia) recruited into a prospective natural history cohort at two adult Sickle Cell Centers. Patients were enrolled during routine clinic visits and in a non-crisis, "steady state". We excluded patients with bone marrow or kidney transplant, diabetic nephropathy, hepatitis B or C, HIV, lupus or other glomerular diseases and those on dialysis. We collected data on treatment including use of hydroxyurea and ACE-inhibitors or angiotensin receptor blockers (ACE-I/ARB). Opioid exposure was determined from state narcotic databases for each patient during the year preceding enrollment. Clinical laboratory tests, including spot urine albumin-creatinine ratio (UACR), were acquired at the baseline visit. Patients were considered to have albuminuria if UACR was ≥30mg/g creatinine. Total opioid use, converted to morphine-equivalent units, was quantified in the preceding 1 month, 6 months, and 12 months. Morphine exposure in each time interval was categorized into three groups for analysis: no morphine exposure, exposure ≤50thpercentile, and exposure >50thpercentile. We used multivariable logistic regression models to assess the relationship between opioid use categories and presence of albuminuria adjusting for the following covariates: age, sex, hydroxyurea use, ACE-I/ARB use, total bilirubin, direct bilirubin, hemoglobin, white blood cell (WBC) count, systolic and diastolic blood pressure, hemoglobin F%, estimated glomerular filtration rate (eGFR) and site of enrollment.
Results:
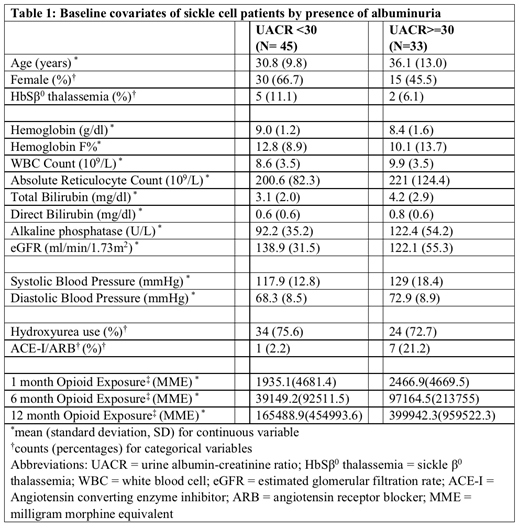
Seventy-eight patients with sickle cell anemia who had complete data for the variables of interest and outcome were included. Mean age was 33.1 years (SD 11.5) and 45 (57.7 %) were female. When comparing patients by albuminuria status (Table), patients with albuminuria were older (36.1 v 30.8 years) and less likely to be female (45.5 % v 66.7 %). Patients with albuminuria had both higher systolic and diastolic blood pressures. Hydroxyurea use was similar between both groups, but albuminuria patients were more likely to receive ACE-I/ARB therapy. Patients with albuminuria were more likely to have lower hemoglobin, higher total bilirubin, alkaline phosphatase and absolute reticulocyte count. Patients with albuminuria also had lower eGFR and greater opioid exposure over each of the three time intervals evaluated. Opioid use in the preceding 1 month was not associated with albuminuria in the adjusted model (p=0.6). Opioid use in the preceding 6 months was associated with albuminuria (p=0.02), patients with opioid exposure >50thpercentile (>5500 mg of morphine equivalent) having a 39.1 (95% CI: 2.1, 719.8; p=0.01) higher odds of developing albuminuria compared to those without opioid exposure. Patients with less than the 50thpercentile also trended towards a higher odds of albuminuria (OR 6.3, 95% CI: 0.7, 58.1; p=0.1), but did not reach statistical significance. As estimates for odds of albuminuria were similar for patients with > 50thpercentile and ≤50thpercentile of opioid exposure over twelve months of exposure, we collapsed the categories into "no opioid exposure" vs. "any opioid exposure." Patients with any amount of opioid use over the preceding 12 months had a higher odds of albuminuria (OR 11.0, 95% CI 1.2, 104.4; p=0.04).
Conclusion:
While limited in sample size, our data demonstrate that higher opioid exposure over the preceding 6 months and any opioid exposure in the preceding year were independently associated with albuminuria in patients with sickle cell anemia. These findings suggest that opioid exposure may be associated with kidney disease in patients with SCD. This association warrants additional study given the common use of these agents in SCD.
Derebail:Retrophin: Consultancy; RTI: Honoraria; Novartis: Consultancy. Ataga:Bioverativ: Honoraria, Membership on an entity's Board of Directors or advisory committees; Emmaus Life Sciences: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Research Funding; Modus Therapeutics: Honoraria; Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Global Blood Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal