

Context - Erdheim-Chester disease (ECD) is a rare non-Langerhans cell histiocytosis characterized by tissue infiltration of CD68 (+), CD1a (-) histiocytes in various organs. It has been classified as a myeloid neoplasia since the discovery of the RAS-RAF-MEK-ERK pathway alterations. Angiogenesis displays an important role in neoplastic and inflammatory process. Vascular Endothelial Growth Factor (VEGF) is a major proangiogenic factor. VEGF is expressed by many tumor cells, and was found to be expressed by Langerhans histiocytic cells. Mechanisms of cardiovascular involvement in ECD are still not clear, however we hypothesize that VEGF may contribute to the development of lesions of ECD. We further hypothesize that VEGF serum level could help distinguish different profiles of patients and study their response to treatment.
Patients and Methods - We conducted a retrospective study in patients with ECD seen in the French National Reference Center for Histiocytoses of the Pitié-Salpêtrière Hospital. These patients had histologically confirmed ECD and were included in the study if they had at least one determination of serum VEGF. Serum VEGF level was assessed by ELISA and considered high when above a concentration of 500pg/mL. Evaluation of cardiac and vascular involvements was based on cardiac magnetic-resonance imaging and CT-angiography of the aorta as often as possible, and replaced by other imaging modalities when they were contraindicated.
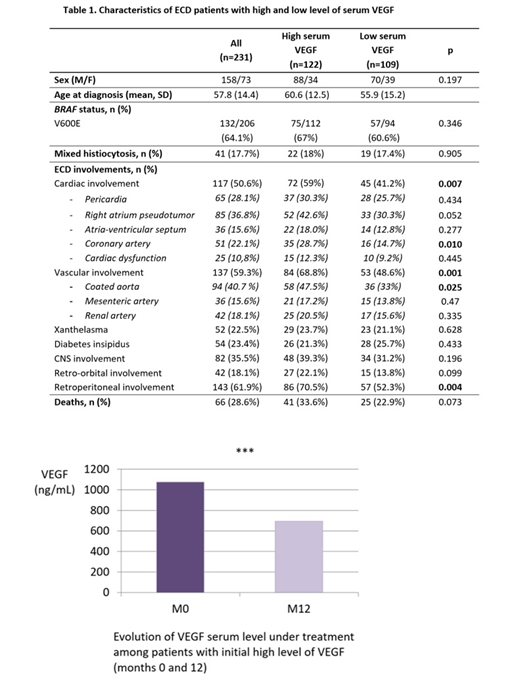
Results - We screened 254 patients of whom 231 had had at least one determination of VEGF serum level. Serums VEGF were high in 122 out of 231 patients (52.8%). Patients with a high serum VEGF level had more frequently a vascular involvement of ECD (68.8% vs 48.6%, p=0.001), especially signs of a "coated aorta" (47.5% vs 33%, p=0.025). Cardiac involvement was also more prevalent in patients with high serum VEGF level (59% vs 41.2%, p=0.007). Notably, coronary arteries were twice as frequently affected (28.7% vs 14.7%, p=0.010). BRAF status was not significantly different between patients with high or low levels of VEGF. VEGF level were not correlated to the presence of an inflammatory syndrome (evaluated on CRP elevation).
At first determination, median serum VEGF among patients with high levels was 850pg/mL (SD 682.22). Under treatment, we observed a decrease of the serum VEGF level. Among 68 patients with a serum VEGF level determination at 12 months, the concentration of VEGF decreased significantly (mean difference 305.4, p<10-6), reaching a median of 507pg/mL (SD 552.58) at 12 months.
Conclusion - Cardiovascular involvement is frequent and prognostically relevant in ECD. Evaluation of ECD clinical course and response to treatment is still challenging, and repeated imaging is often necessary. VEGF serum level could help distinguish patients with cardiovascular profile and contribute to follow up under treatment. Comprehension of the role of VEGF and the possible impact of anti-VEGF treatment will benefit from a study of VEGF and VEGF-receptor expression in lesions of ECD patients.
No relevant conflicts of interest to declare.

