

Several therapeutic approvals in recent years have resulted in a change in the paradigm for standard treatment of patients with newly diagnosed and relapsed/refractory (r/r) AML. Gemtuzumab ozogamicin (GO) was resurrected in 2017 for CD33+ newly diagnosed or relapsed/refractory AML using a safer fractionated dosing regimen. Since its re-approval it has been incorporated in combination with standard 7+3 (cytarabine 100mg/m2 + daunorubicin 60mg/m2; Castaigne S et al, Lancet 2012) as upfront therapy for good and intermediate risk AML patients (pts) treated at institutions with access to rapid risk stratification (molecular/cytogenetic results) including ours (Roswell Park; RP). In the five randomized studies of GO combinations for newly diagnosed AML, varied doses of cytarabine and anthracyclines were used (Lancet Oncol, 2014). In these, cytarabine doses ranged from (100-200 mg/m2), daunorubicin doses ranged from 45-60 mg/m2. These studies did not intensify daunorubicin beyond 60mg/m2 and did not incorporate FLT3 inhibitors. Previous work has demonstrated that anthracycline dose intensification (90mg/m2) provides a recognized survival advantage for younger AML pts (Luskin MR et al, 2016.), particularly those with mutations in FLT3. Optimal combination approach(s) including GO for the management of patient with AML are unclear.
Adaptation of GO in combination with 7+3 for upfront AML management has led to the evolution of institutional standards to optimize early identification of good/intermediate risk AML pts. Unfortunately, there is limited data on the safety and efficacy of higher doses of daunorubicin in combination with GO and/or FLT3 inhibitors. Here we present outcomes and adverse events (AEs) using varied upfront treatment regimens in combination with GO at RP. We additionally present a cohort of r/rAML pts treated with GO alone or in combinations under an expanded access protocol (NCT02312037) at RP prior to re-approval in 2017. R/R AML pts treated on expanded access had AEs collected prospectively, all other cases were identified by retrospective chart review in accordance to IRB approval.
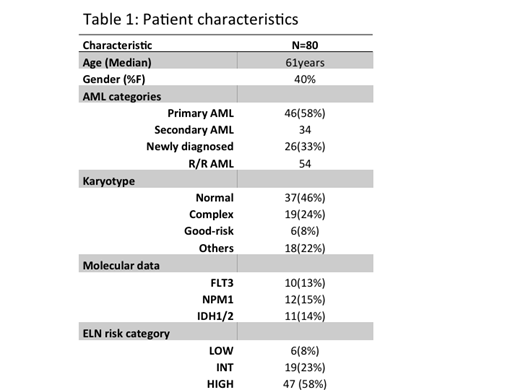
218 patients with a diagnosis of AML and a median age of 66.5 years were seen at RP since GO approval. Of these all good risk and 45% of intermediate risk AML underwent induction chemotherapy. During 2015-2017 r/rAML patients were treated with GO based therapy (N=32) on NCT02312037 trial. Since FDA approval another 48 pts have been treated with GO at our institution. Of the 80 patients in this cohort, N=25 underwent GO based induction therapy (Table 1). The most frequently used other combinations were: (i) daunorubicin 60mg/m2 and cytarabine 200mg/m2 (N=17), (ii) daunorubicin 90mg/m2 + cytarabine 100mg/m2, N=4), (iii) FLAG-GO (used in patients with cardiac comorbidities; N=2) and hypomethylating agents combined with GO (N=10), monotherapy was used in 45 pts. The ORR (CR+Cri) for patients treated with GO based induction was 88%. The overall (OS) and event free survival (EFS) were 48 and 17 months for induction-treated pts respectively. The most common AEs were febrile neutropenia (60%), infusion reactions (30%), transaminitis (20%), cytopenias beyond 30 days from induction (10%). The most common reason for change of therapy was disease progression. Toxicity was not higher in those patients receiving higher doses (>60mg/m2) of daunorubicin or cytarabine (200mg/m2). Two patients received GO+7+3+FLT3 inhibitors; this was well- tolerated in a very small sample. In the R/R cohort, pts received a median of 2 cycles of therapy, the ORR was 18%. GO had no activity in those treated with >2 prior regimens for relapsed disease.
In conclusion, anthracycline intensification as part of a 7+3 combination with GO was not associated with increased toxicity. Although the number was small, FLT3 inhibitors following 7+3+GO were also well tolerated. These data require confirmation in a larger cohort. Our results confirm the EFS reported in the literature (18 months in ALFA 0701 study), and suggest a higher mean OS of 40 months compared with conventional 7+3 induction. The response rate for GO monotherapy in r/rAML is low and was exceedingly poor for heavily pretreated pts.
Thota:Incyte, Inc.: Speakers Bureau. Griffiths:Novartis Inc.: Consultancy; Appelis Pharmaceuticals: Other: PI on a clinical trial; Onconova Therapeutics: Other: PI on a clinical trial; Partner Therapeutics: Consultancy; Astex Phramaceuticals/Otsuka Pharmaceuticals: Consultancy, Research Funding; Astex Phramaceuticals/Otsuka Pharmaceuticals: Consultancy, Research Funding; New Link Genetics: Consultancy; New Link Genetics: Consultancy; Persimmune: Consultancy; Persimmune: Consultancy; Boston Scientific: Consultancy; Boston Scientific: Consultancy; Abbvie, Inc.: Consultancy; Partner Therapeutics: Consultancy; Novartis Inc.: Consultancy; Appelis Pharmaceuticals: Other: PI on a clinical trial; Abbvie, Inc.: Consultancy, PI on a clinical trial; Celgene, Inc: Consultancy, Research Funding; Celgene, Inc: Consultancy, Research Funding; Onconova Therapeutics: Other: PI on a clinical trial; Genentech, Inc.: Research Funding; Genentech, Inc.: Research Funding. Wang:Agios: Other: Advisory role; Abbvie: Other: Advisory role; Kite: Other: Advisory role; Jazz: Other: Advisory role; Amgen: Other: Advisory role; Daiichi: Other: Advisory role; Astellas: Other: Advisory role, Speakers Bureau; celyad: Other: Advisory role; Pfizer: Other: Advisory role, Speakers Bureau; Stemline: Other: Advisory role, Speakers Bureau.

