

Introduction. Intra-tumoral T-cell infiltration is associated with R-CHOP responsiveness in aggressive B-cell lymphoma (Keane, Lancet Haem 2015). These patients also have a broad (i.e. diverse) intra-tumoral T-cell receptor (TCR) repertoire with a ~20% superior survival compared to those with a narrow (i.e. clonal) repertoire after R-CHOP therapy. Here, the major contributor to the TCR clonal expansion were CD8+ T cells (Keane, CCR 2017). Paradoxically, our recent results in Follicular Lymphoma (FL) (Tobin, JCO in press) found that clonal T-cell expansions were markedly enriched in those patients that experienced progression of disease within 24 months (POD24). Given that FL is a histological subtype associated with a tumor microenvironment distinct from DLBCL including numerous CD4+ T-follicular helper cells (TFH), we now expand upon these findings by comparing TCR repertoires across histological subtypes. We then established whether the TCR repertoire in FL is related to differential TCR clonal expansions between different T-cell subsets and immune checkpoints. Finally, the overlap between tissue and blood TCR repertoires was investigated.
Methods. Firstly, unbiased, high-throughput TCRβ sequencing (ImmunoSEQ, Adaptive Biotechnologies) was compared in 164 FFPE tissues (12 healthy nodes, 40 FL, 88 DLBCL, and as a comparator tumor known to be sensitive to checkpoint blockade and to have a high neoantigen burden, 24 melanoma tissues). Next, to determine the contribution of individual T-cell subsets to overall clonality, a further 21 fresh de-aggregated/cryopreserved FL tumor samples were FACS sorted into four T-cell groupings: CD8+ cytotoxic T-lymphocytes (CTLs), CD4+ TFH, CD4+ regulatory T-cells (TREGs) and 'other' (non-TFH/TREG) CD4+ T-cells. Flow cytometry quantified the expression of the checkpoints LAG3, TIM3 and PD1. Then, 5 FL paired tissue/blood samples were tested for shared TCR clones.
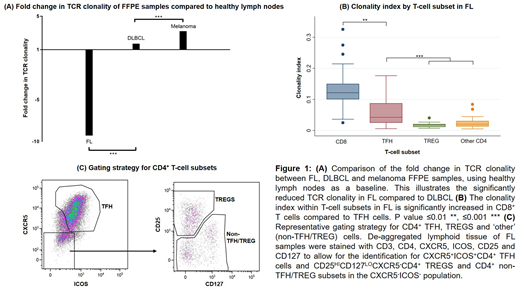
Results. FL exhibited strikingly reduced TCR repertoire clonality (higher diversity) compared to DLBCL, melanoma and healthy lymph nodes (Fig 1A). Analysis of de-aggregated sorted nodal T-cells revealed a more complex TCR repertoire. The outcome measure was median clonality index (CIx ranging from '0' or minimal, to '1' or maximal clonality). Large T-cell clones in FL (CIx=0.12) predominantly resided within the CTL subset (34% all T-cells). By contrast, there was marked T-cell diversity in TFH (CIx=0.04; 27% all T-cells), TREG (CIx=0.02; 7% all T-cells) and 'other' CD4+ T-cells (CIx=0.02; 32% all T-cells) (Fig 1B). The CTL population had a bimodal expression for PD1 (+51%/-49%), a marker in FL that has been shown to remain functionally active unless co-expressed with LAG3 and/or TIM3 (Yang, Oncotarget 2017). These dual-checkpoint expressing CTLs have reduced capacity to produce cytokines or lytic granules (i.e. they are 'exhausted'). Notably, 54% of the PD1+ CTLs co-expressed either LAG3 or TIM3. Put together, these results are consistent with expanded CTL clones that are frequently functionally exhausted.
In contrast, TFH, TREG and 'other' CD4+ T-cells had a low expression of LAG3 and TIM3, although PD1 was frequently found (as expected, particularly in the TFH cells). Finally, in paired tissue/blood samples, there was weak overlap between the circulating and intra-tumoral TCR repertoire in CTLs and TFH T-cells.
Conclusion. Although FL has a markedly less clonal TCR repertoire compared to DLBCL, melanoma and even healthy nodes, this result is misleading. Detailed analysis on sorted intra-tumoral T-cell subsets in FL revealed large clonal expansions in CTLs, with approximately half of these classified as functionally exhausted (dual-positive for PD1 and LAG3 and/or TIM3), a state potentially amenable to reversal by dual-checkpoint blockade. The explanation for TCR repertoire diversity lies in CD4+ T-cells (representing approximately two-thirds of T-cells, including the large TFH subset). T-cells in blood did not reflect FL tissue T-cell clones, further highlighting the need for sorted intra-tumoral nodal tissues to accurately assess TCR repertoires in FL. Further characterization of the neo-antigenic targets that CTL clones potentially recognize is required. These results have implications for therapeutic vaccine design and selective recruitment of patients for immune checkpoint blockade.
Keane:MSD: Consultancy; Gilead: Consultancy; Celgene: Consultancy; Roche: Consultancy, Other: Travel Grant; BMS: Research Funding. Gandhi:Roche: Honoraria, Other: Travel Support; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Merck: Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria; Bristol Myers Squibb: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Gilead: Honoraria, Research Funding.

