

Resetting the immune system through autologous hematopoietic stem cell transplant (autoHSCT) is a highly effective treatment in selected patients with autoimmune diseases. AutoHSCT can induce long-term remission (up to 15 years) with 70-80% progression free survival in patients with relapsed refractory and secondary progressive multiple sclerosis (Muraro 2017) that is superior to standard of care agents in a randomized study (Burt 2019). Likewise, use of autoHSCT in scleroderma patients achieved superior outcomes in two randomized studies (Tyndall 2014, Sullivan 2018). These impressive results are achieved by a combination of the eradication of autoreactive immune effector cells and re-establishment of a self-tolerant immune system, i.e., immune system reset. However, only a small fraction of eligible patients undergo autoHSCT, in part due to toxicity associated with current conditioning protocols. To address these issues, we are developing antibody drug conjugates (ADCs) that selectively target CD45 to eradicate autoimmune cells and enable autoHSCT as a potential one-time curative treatment for patients with autoimmune disease.
To model this approach in mice, we generated an anti-mouse CD45 ADC that was evaluated for the ability to condition recipients in a murine congenic transplant model following a single myeloablative dose. This ADC was further evaluated for its ability to eliminate pathogenic host-reactive cells and enable immune reset in recipients in multiple murine models of autoimmune disease, including MOG-induced experimental autoimmune encephalitis (EAE), proteoglycan-induced arthritis (PGIA), and sclerodermatous graft-vs-host disease (scGVHD).
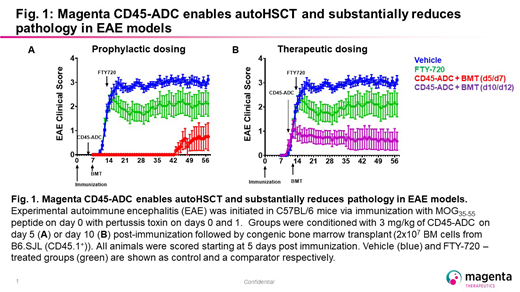
A single-dose of tool anti-mouse CD45-ADC at 3 mg/kg achieved full myeloablation in recipient mice (>99% depletion of LT-HSCs (Lin-Kit+Sca-1+CD150+CD48-). Transplanted mice achieved full engraftment with congenic BMT (>90% chimerism at 16 weeks). In EAE, conditioning with a non-myeloablative dose of the CD45-ADC followed by congenic transplant prior to disease onset significantly delayed disease onset and reduced disease severity (onset at 21 days, peak disease score 2.1 for with 1 mg/kg CD45-ADC; onset at 42 days, peak disease score 0.75 for 3 mg/kg CD45-ADC + BMT; onset at 11 days with peak disease score 3.1 for vehicle-treated)[Figure 1]. In active EAE, treatment with 3 mg/kg of CD45-ADC on day 10 or 13 followed by congenic transplant halted progression of disease activity (no increase from disease score at time of treatment; peak disease scores of 0.75 and 2.3, respectively). The effect observed with CD45-ADC treatment at day 13 with congenic transplant was comparable to that achieved by treatment with a clinically validated standard of care, FTY-720 (approved S1P1 antagonist equivalent to Gilenya) at day 13 which also halted disease at a peak score of 2.3. Disease control in this study compared favorably to a prior study where mice were treated with 9 Gy TBI + congenic BMT at day 9. These data show that CD45-ADC conditioning followed by congenic transplant is effective at immune reset and shows comparable efficacy to clinically validated therapies. Evaluation of this ADC in additional autoimmune models of arthritis and scleroderma are ongoing and will be presented.
To translate these encouraging pre-clinical data, we generated novel anti-human CD45 ADCs that cross react with nonhuman primates (NHP) and evaluated these for the ability to deplete hematopoietic and immune cells in vitro and in vivo in humanized NSG (hNSG) mice. The CD45-ADC showed efficient killing of human BM CD34+ (EC50 2.44 x 10-9 M) and peripheral CD3+ cells from normal donor (EC50 7.6 x10-10 M) and MS patients (EC50 1.5 x 10-10 M). In vivo in hNSG, single doses of the CD45-ADCs were well-tolerated and led to substantial (>95%) depletion of human cells. In NHPs, single doses of CD45-ADCs were well tolerated and achieved >90% peripheral lymphocyte depletion and >80% depletion of HSCs. Dose escalation studies are continuing and will be reported.
These results suggest that targeted immune depletion with a single treatment of CD45-ADC may be sufficient for auto-HSCT and allow immune reset and re-establishment of immune tolerance. Targeted CD45-ADCs may represent a safer and better tolerated approach for conditioning patients prior to immune reset through autoHSCT and may significantly reduce the side effects associated with current conditioning.
Gillard:Magenta Therapeutics: Employment, Equity Ownership. Proctor:Magenta Therapeutics: Employment, Equity Ownership. Brooks:Magenta Therapeutics: Employment, Equity Ownership. Lamothe:Magenta Therapeutics: Employment, Equity Ownership. Hyzy:Magenta Therapeutics: Employment, Equity Ownership. Mikse:Magenta Therapeutics: Employment, Equity Ownership. McDonough:Magenta Therapeutics: Employment, Equity Ownership. Palchaudhuri:Magenta Therapeutics: Employment, Equity Ownership. Bhat:Magenta Therapeutics: Employment, Equity Ownership. Sarma:Magenta Therapeutics: Employment, Equity Ownership. Bhattarai:Magenta Therapeutics: Employment, Equity Ownership. Sawant:Magenta Therapeutics: Employment, Equity Ownership. Pearse:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties. Mcdonough:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties. Boitano:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties. Cooke:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties.

