

Background:
Immunocompromised patients (pts) face an approximate 6-fold increase in lifetime risk of lymphoid malignancies compared with immunocompetent counterparts. Additionally, up to 80% of post-transplant lymphoproliferative disease (PTLD) cases are driven by EBV-associated mechanisms of tumorigenesis. Approximately 70% will express CD30 and over 80% will express CD20. Recent studies of chemoimmunotherapy (CIT) have reported median overall survival (OS) of 2-4 years and treatment-related mortality (TRM) rates of 13-50%. Moreover, solid organ transplant (SOT) pts are at significant risk of graft rejection when CIT is employed, possibly due to "off target" depletion of regulatory T-cell populations. R monotherapy induction, followed by response-stratified use of CIT, has been evaluated (Trappe, et al, JCO, 2016). However, ~75% of pts had an inadequate response to R alone and required subsequent CIT; 2-yr OS for the population as a whole was ~70%. BV is an anti-CD30 antibody-drug conjugate that received accelerated FDA approval for previously untreated CD30+ T-cell lymphoma and Hodgkin lymphoma. We hypothesized that a combination of BV and R would yield improved breadth and depth of response compared with R monotherapy induction, would spare pts subsequent exposure to CIT, and result in favorable OS.
Methods:
We report here results of a phase I/II multicenter study investigating the efficacy and safety of BV+R as frontline therapy in pts diagnosed with immunosuppression-associated CD30+ and/or EBV+ lymphoid malignancies. Induction consisted of R 375 mg/m2 given days 1, 8, 15, 22 and BV 1.2 mg/kg given days 1, 8, 15, of a 28-day cycle, followed by restaging. Those with progression were removed from study. Pts with stable disease were offered study discontinuation or completion of one consolidation cycle followed by repeat disease assessment. Pts with partial response or complete response (CR) could receive either consolidation followed by maintenance therapy (MT) or move directly to MT without consolidation. Consolidation was identical to induction dosing; MT consisted of BV 1.8 mg/kg every 3 weeks and R 375 mg/m2 every 6 weeks for up to 1 year of therapy. Toxicity was defined using CTCAE 4.0 and response (Cheson, 2007) was assessed at the end of induction, consolidation (if given), and after cycles 4 and 7 of BV.
Results:
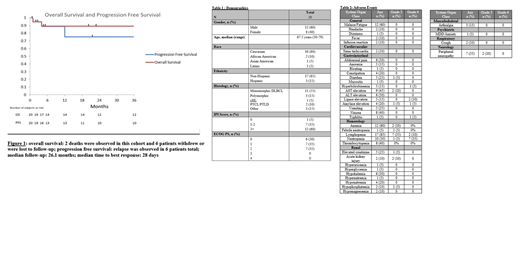
A total of 22 pts were entered in the trial. Toxicity and response data are available for 20 pts. Median age was 67 years (range, 30-79) and 14 pts (64%) were male (range, 30-79 years). Fourteen pts (64%) had received either a SOT or hematopoietic allograft requiring immunosuppression, 3 pts required immunosuppression for underlying rheumatologic conditions, and 3 pts were found to have EBV-associated lymphoid malignancies in the absence of iatrogenic immunosuppression (Table 1). Overall response rate was 70%, including a CR rate of 60%. With median follow-up of 26.1 month, the probability of progression-free survival at 1 year was 75.2% and 67.6% at 3 years (Fig 1). Probability of OS was 89.2% at both 1-year and 3-year follow-up (Fig 1). Median time to best response was 28 days. Three pts withdrew consent after induction, 2 pts died (1 death related to treatment), and 1 patient was lost to follow-up. Seven pts (31%) required dose adjustments or delay of medication administration during induction therapy and 45% required discontinuation of therapy due to toxicity within 1 year. The most frequent grade 3/4 toxicities were peripheral neuropathy, neutropenia, lymphopenia, and pancreatitis. The most frequent adverse events of any grade were fatigue, nausea, abdominal pain, pancytopenia, and peripheral neuropathy (Table 2).
Conclusions:
The combination of BV + R had an acceptable safety profile and appeared effective in achieving early remissions when used as frontline therapy for PTLD and other immunosuppression-related lymphomas. Specifically, over half of pts achieved CR, and 75% have been spared exposure to multi-agent cytotoxic chemotherapy. Furthermore, survival and PFS data were encouraging compared with historical controls. However, nearly half of pts discontinued therapy within 1 year due to toxicity suggesting poor long-term tolerance of the regimen and that earlier cessation of therapy may be warranted. Further studies are needed to confirm these efficacy results and to determine optimal BV+R dosing regimens and durations.
Pro:Seattle Genetics: Consultancy, Honoraria, Other: Travel Expenses, Research Funding; Takeda: Consultancy, Honoraria, Other: Travel Expenses; Celgene: Consultancy, Honoraria; Kyowa Hakka Kirin: Consultancy, Honoraria. Gordon:Gilead: Other: Advisory Board; Bayer: Other: Advisory Board; Juno/Celgene: Other: Advisory Board, Research Funding; Zylem LLC: Other: co-founder; research in nanoparticles in cancer. Karmali:Gilead/Kite; Juno/Celgene: Consultancy, Speakers Bureau; Astrazeneca: Speakers Bureau; Takeda, BMS: Other: Research Funding to Institution. Winter:Merck: Consultancy, Research Funding. Ma:Astra Zeneca: Consultancy, Research Funding, Speakers Bureau; Xeme: Research Funding; Bioverativ: Consultancy; Beigene: Research Funding; Pharmacyclics: Consultancy, Research Funding, Speakers Bureau; Kite: Consultancy; Janssen: Consultancy, Speakers Bureau; Genentech: Consultancy; Abbvie: Research Funding; Incyte: Research Funding; Juno: Research Funding; Acerta: Research Funding; Gilead: Research Funding; Novartis: Research Funding. Behdad:Pfizer: Other: Speaker; Thermo Fisher: Membership on an entity's Board of Directors or advisory committees; Loxo-Bayer: Membership on an entity's Board of Directors or advisory committees. Petrich:AbbVie: Employment, Equity Ownership. Smith:Portola Pharmaceuticals: Research Funding.

