


Salvage options for children with relapsed ALL remain sub-optimal, particularly for T-cell ALL patients, and relapse remains the leading cause of death. Achieving complete remission (CR) after relapse is the first critical step to cure. Combining the proteasome inhibitor (PI) bortezomib with chemotherapy has previously shown promising results in achieving CR in pediatric phase 2 studies in ALL (Messinger 2012, Horton 2013, Bertaina 2017).
In this ongoing dose-escalation phase 1 study, the second generation PI carfilzomib was combined with chemotherapy in children with relapsed ALL. Subjects received one 4-week cycle of induction chemotherapy with either UKALLR3 (dexamethasone, mitoxantrone, methotrexate, PEG-asparaginase, vincristine) or VXLD (vincristine, dexamethasone, PEG-asparaginase, daunorubicin) plus carfilzomib administered intravenously on days 1, 2, 8, 9, 15, and 16. The primary endpoint was dose limiting toxicities (DLTs) occurring during induction (grade 4 neutropenia or thrombocytopenia extending past day 45 or grade 4 non-hematological toxicity). Efficacy endpoints included CR (with or without hematological recovery) based on bone marrow (BM) and LP on day 29 of induction and consolidation. Subjects < 21 years of age and diagnosed with first early BM relapse (<36 months from diagnosis), multiply relapsed ALL, or primary induction failure were eligible; subjects with T-cell disease with any BM relapse were eligible. Subjects achieving ≥ stable disease could receive a cycle of modified BFM consolidation therapy (6-MP, cyclophosphamide, cytarabine, PEG-asparaginase, IT chemotherapy) plus carfilzomib at the same dose level and schedule given in induction therapy. Dose escalation was based on an evaluation of DLT's using a Bayesian logistic regression model.
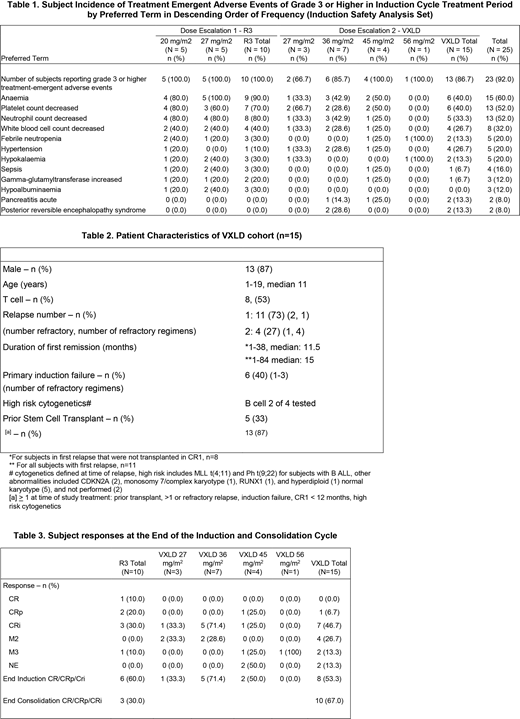
Ten subjects with B (n=9) or T- (n=1) cell ALL were treated with UKALLR3 at 2 carfilzomib dose levels (20 or 27 mg/m2, 5 subjects each). Among DLT-evaluable subjects, 3 DLTs (meningoencephalitis, hemolytic uremic syndrome and neutropenia) were observed, 2 at 27 and 1 at 20 mg/m2 dose levels with an MTD of 27 mg/m2. The UKALLR3 regimen was considered too toxic by the protocol steering committee and was replaced with VXLD in January 2016. The VXLD cohort started at 27 mg/m2 and is currently in the 56 mg/m2 dose level. Fifteen subjects (7 B-cell and 8 T-cell) were treated with VXLD at carfilzomib dose levels of 27 (n=3), 36 (n=7), 45 (n=4), and 56 (n=1) mg/m2. One DLT of posterior reversible encephalopathy syndrome (PRES) occurred in the 36 mg/m2 cohort, with no further DLTs identified after expansion to 7 subjects. Table 2 lists the patient characteristics of the 15 subjects in the VXLD cohort.
Grade 3-4 hematological AEs were nearly universal for both UKALLR3 and VXLD. Non-hematological > Grade 3 AE's of note are listed in Table 1. PRES occurred in 2 subjects in the VXLD cohort (both with prior allogeneic SCT) and rapidly reversed in both cases. Re-challenge with carfilzomib in one case was tolerated without PRES recurrence. Serious AE's (SAE) were reported in 50% and 56% of subjects receiving carfilzomib in combination with UKALLR3 or VXLD, respectively, with the most common SAE's among all subjects being sepsis (16%), pancreatitis and PRES (8% each).
In the UKALLR3 cohort, 60% of subjects (n=6) achieved a remission, however only 30% proceeded to consolidation. In the VXLD cohort, 53% of evaluable subjects (n=8) achieved remission and 13% were non-evaluable due to hypocellular BM at day 29 of induction. All responding subjects recovered hematological counts by day 42 without evidence of progression. Eight subjects (53%) proceeded to consolidation, including 2 subjects with non-evaluable BM results and 1 with 8% BM blasts after induction. All subjects entering consolidation were in remission on day 29 post-consolidation. The overall remission rate with VXLD-carfilzomib was 67% at the end of consolidation. Detailed response data are listed in Table 3.
Carfilzomib in combination with VXLD chemotherapy was tolerable in a predominantly T-cell ALL population, very early or post stem cell transplant relapse. Efficacy is promising in this small cohort of patients with carfilzomib dose escalation continuing.
Burke:Amgen, Inc.: Consultancy, Speakers Bureau. Bautista Sirvent:EusaPharma: Consultancy, Membership on an entity's Board of Directors or advisory committees, Other: Support for attending symposia; Takeda: Other: Support for attending symposia; Bayer: Consultancy, Membership on an entity's Board of Directors or advisory committees; Jazz Pharmaceuticals: Honoraria, Other: Support for attending symposia; Amgen, Inc.: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees. Gore:Amgen: Consultancy, Equity Ownership, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel expenses; Novartis: Consultancy, Other: Service on Data Safety Monitoring Committee; travel, accommodations, expenses; Roche/Genentech: Consultancy, Honoraria, Other: travel expenses; Anchiano: Equity Ownership, Other: spouse employment and company leadership; Blueprint Medicines: Equity Ownership; Celgene: Equity Ownership, Other: DSMC member; Clovis: Equity Ownership; Mirati: Equity Ownership; Sanofi Paris: Equity Ownership. Locatelli:Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Miltenyi: Honoraria; bluebird bio: Consultancy; Bellicum: Consultancy, Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees. O'Brien:BMS: Research Funding; Celgene: Research Funding; Pfizer: Research Funding; AbbVie: Research Funding; Amgen: Research Funding; BTG: Research Funding. Obreja:Amgen, Inc.: Employment, Equity Ownership. Morris:Amgen, Inc.: Employment, Equity Ownership. Baruchel:Novartis: Consultancy, Honoraria; Servier: Consultancy, Honoraria; Bellicum: Consultancy; Celgene: Consultancy, Honoraria.
Kyprolis is a proteasomal inhibitor indicated in combination with dexamethasone or with lenalidomide plus dexamethasone for the treatment of patients with relapsed or refractory multiple myeloma who have received one to three lines of therapy. It is also indicated as a single agent for the treatment of patients with relapsed or refractory multiple myeloma who have received one or more lines of therapy.
This icon denotes a clinically relevant abstract

