

Background
Waldenström's macroglobulinaemia (WM) is a rare non-Hodgkin B cell lymphoma. Given its rarity, information about both patient demographics and disease characteristics are limited. Treatment is indicated for symptomatic patients and treatment regimens have evolved significantly in recent years. The Rory Morrison Registry (RMR) has comprehensive patient data available for analysis. We seek to draw conclusions about UK patient demographics and disease characteristics, and evaluate how treatment practices have evolved.
Methods
The RMR was searched for all patients with a diagnosis of WM. Patient demographics, disease characteristic, pathology results, treatment information and survival status retrieved. Kaplan Meier and log rank analysis was performed.
Results
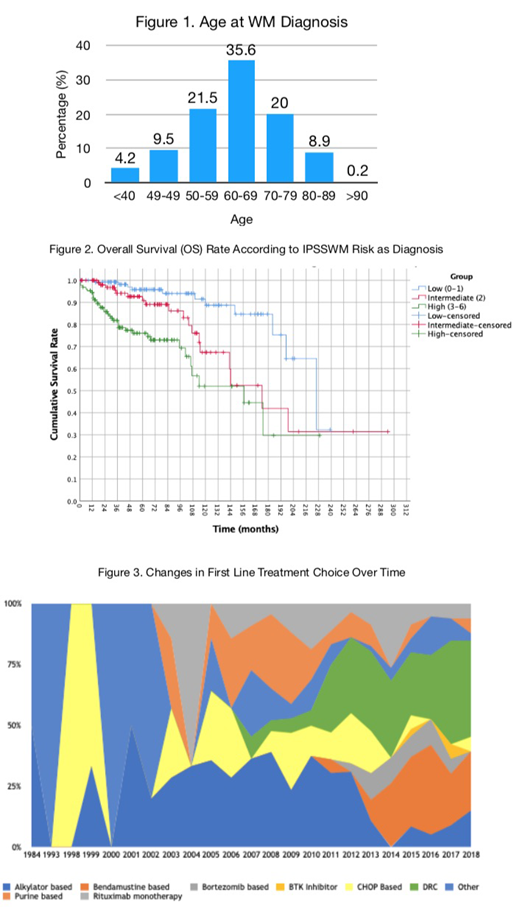
671 patients were identified from 19 different UK centres. Median age at diagnosis was 64 years (range 27-92, figure 1). Year of diagnosis ranged from 1978 to 2019, with 7 patients diagnosed <1990, 31 1990-1999, 200 2000-2009, and 433 since 2010. Male to female ratio was 1.62:1. 90.4% were Caucasian, 5.9% Asian, 1.3% Afro-Caribbean, 0.7% mixed, and 1.6% of other ethnicity.
Median haemoglobin at diagnosis was 112g/L (range 33-170), platelet count 242 (3-806), B2M 3 (range 0.2-56.3) and M-protein 17g/L (range 0-110.5). Median bone marrow infiltration was 40% (range 0-100%), with 35% lymphocytes and 5% plasma cell. MYD88 L265P mutations were detected in 160/190 patients (84.2%). CXCR4 mutations, for which testing is not widely available, were detected in 20/76 patients (26.3%). Peripheral neuropathy was seen in 74 patients, with 28 anti-MAG antibody positive. Other manifestations at diagnosis included cryoglobulinaemia (26), amyloidosis (12) and Schnitzler's syndrome (7). 2/317 patients were HIV positive, 4/341 HCV antibody positive, 27/334 HBSAb positive, and 12/327 HBCAb positive. IPSSWM score at diagnosis was available for 352 patients, with a low score in 122 (34.7%), intermediate score in 103 (29.3%), and high score in 123 (45%).
440 patients (65.6%) had received treatment, with a median time from diagnosis to treatment of two months (range 0-312). Indications for first line treatment initiation were: 35% paraprotein-related, 30% lymphoma-related , 2.1% B-symptoms, and a combination of indications for the remainder. Hyperviscosity was the treatment indication in 24.8% of patients, fatigue in 21.6% and peripheral neuropathy in 9.8%. At treatment commencement, 47% of patients had a haemoglobin of <100g/L. CNS involvement was a feature in 1.5% and 1.5% high grade transformation (HGT).
Lines of therapy received was one in 43.6%, two in 24.1%, three in 4.8%, four in 6.6% and ≥5 in 10.9%. In the past decade, 27.8% received DRC, 16.4% R-Bendamustine, 8.9% rituximab monotherapy, 7.7% R-CHOP and the rest varying combinations. 2.2% had received Bortezomib-containing therapy. Before 2010, chlorambucil (21.8%), R-CHOP (10.9%) and FC (9.3%) were the most frequently used first line treatments. BTK-inhibitors have become the most commonly used second line therapy, representing 23% of second line therapy after 2010, reflecting the availability of Ibrutinib on the Cancer Drugs Fund from 2017 and the availability of BTKi trials since 2015. 88 patients had received a BTKi at some point.
118 patients had deceased. Only 30 patients had a cause of death available; this included 7 patients who died from WM itself, 6 from pneumonia, 5 from sepsis (2 were neutropaenic), 3 from HGT, 2 from haemorrhage, 2 from thrombotic events, and 1 from CNS relapse. 5- and 10-year OS rates from diagnosis were 90.5% and 79.4%, with a significant difference in OS rates according to IPSSWM risk at diagnosis (p<0.001, figure 2). There was a trend towards difference in OS rates (P=0.095) according to MYD88 status, with somewhat poorer OS rate amongst MYD88 wild-type patients. CXCR4-status did not impact the OS rate (p=0.93).
Conclusions
The median age at diagnosis was 64 years, with a third of patients diagnosed under the age of 60. Although diverse, the most frequent indications for treatment in this cohort are hyperviscosity, fatigue and peripheral neuropathy. OS rates are high and correlate with IPSSWM risk, but a majority of patients had received multiple lines of therapy reflecting the chronically relapsing nature of WM. Treatment practices are clearly evolving, with increasing first line use of DRC and R-Bendamustine, as well as BTK inhibitors for relapsed disease.
McCarthy:Janssen: Honoraria, Other: Educational grant to attend meetings . Pratt:Binding Site, Amgen, Takeda, Janssen, Gilead: Consultancy, Honoraria, Other: Travel support. D'Sa:Janssen: Honoraria, Research Funding.

