

Introduction:
Relapsed and refractory aggressive B-cell lymphomas can be cured with hematopoietic stem cell transplant (HSCT), but effective salvage regimens are required. Anthracyclines are the most effective agents in lymphoma and dose-adjusted doxorubicin, etoposide, vincristine, cyclophosphamide, prednisone with rituximab (DA-EPOCH-R) was originally developed in relapsed/refractory lymphomas. Gene-expression profiling of diffuse large B-cell lymphoma (DLBCL) identified stromal signatures associated with inferior survival and targeting the tumor microenvironment may block important survival signals. Alemtuzumab is a humanized monoclonal antibody targeting CD52, present on both B and T-cells. We hypothesized that targeting CD52 could overcome treatment resistance. We report the safety and activity of alemtuzumab added to DA-EPOCH-R in relapsed/refractory aggressive B-cell lymphomas, including Hodgkin lymphoma (HL).
Methods: Adult pts with relapsed/refractory aggressive B cell lymphomas and adequate organ function were eligible. Pts with HIV or CNS involvement were ineligible. Pre-treatment evaluation included laboratory investigations, computed tomography (CT) scans, bone marrow aspirate/biopsy, and brain MRI/CT if indicated. Alemtuzumab 30 mg was infused first on day 1 over 12 hours before rituximab. EPOCH was infused over 5 days and dose-adjusted based on neutrophil nadir for up to 6 cycles. Responding pts were allowed to receive consolidation. Infective prophylaxis included trimethoprim-sulfamethoxazole, acyclovir, and fluconazole in all pts, and lamivudine for pts at risk of HBV reactivation. PCR for cytomegalovirus (CMV) was done at baseline and with every cycle. Tumor response was assessed per the revised 2014 International Working Group guidelines. CT scans were performed after cycles 4 and 6, and every 3 months for year 1, 4 months for year 2 and 6 months for years 3-5. Positron-emission tomography scans were performed after cycle 4 and 6. The primary endpoint of the study was overall response rate.
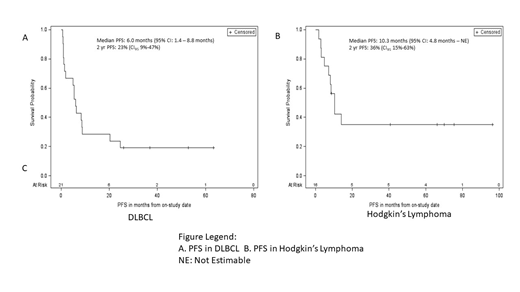
Results: 50 pts were enrolled from November 2009 to March 2014. Two pts did not receive any chemotherapy due to congestive heart failure and rapid disease. 48 pts received 1 cycle and were included in the analysis. Median age was 45 years (range, 18-72) and 29 (60%) pts were male. Twenty-one (44%) pts had DLBCL (T-cell-histiocyte rich DLBCL (THRLBCL) in 4), 16 (33%) HL, 6 (13%) primary mediastinal B-cell lymphoma, 4 (8%) mediastinal grey zone lymphoma and 1 (2%) B-cell lymphoma NOS. Median lines of prior treatment was 2 (range 1-10). All pts received prior anthracycline and 10 (20%) received prior ASCT. Thirty-five (72%) were primary refractory to chemotherapy. In 46 pts evaluable for response, overall response rate (ORR) was 65% including a complete response (CR) rate of 33%. Of 30 responding pts, 13 (44%) received consolidation therapy (5 allogeneic HSCT, 7 radiation, 1 ASCT) and 17 received no further therapy with 7 long-term remissions. In 20 evaluable DLBCL pts, the ORR was 65% including a 30% rate of CR. All 4 THRLBCL responded and 3 had durable remissions after consolidative XRT (2) and allogeneic HSCT (1). In 15 evaluable HL pts, the ORR was 80% including a CR rate of 60%. After a median potential follow up of 84.6 months, median PFS and OS were 6.7 months (CI95: 4.1 - 10.4) and 18.1 months (CI95: 11.5 - not estimable), respectively. In DLBCL, the 2-year PFS and OS were 23% (CI95 9%-47%) (Figure 1A) and 41% (CI95 19%-66%), respectively, while in HL, the 2-year PFS and OS were 36% (CI95 15%-63%) (Figure 1B) and 60% (CI95 33%-82%), respectively. Febrile neutropenia, grade 4 thrombocytopenia, and CMV reactivation without infection occurred in 18%, 26%, and 53% of cycles, respectively. Grade 3 infection occurred in 18% of pts and included BK (3), HSV (1), and CMV (1). Overall, 27 deaths occurred, 3 during therapy (2 of sepsis, 1 of congestive heart failure) and 24 post-therapy (9 of PD, 5 of sepsis, 1 of hemorrhage, 1 of PTLD, and 8 of unknown causes).
Conclusion: Alemtuzumab can safely be added to DA-EPOCH-R in relapsed/refractory aggressive B-cell lymphomas without a significant increase risk of opportunistic infections or unexpected toxicity. Nearly half of patients were successfully bridged to consolidation therapy; however, selected pts, particularly those with significant T-cell infiltration, experience long-term durable remission.
Dunleavy:Pharmacyclics: Membership on an entity's Board of Directors or advisory committees.
Alemtuzumab is not standard of care treatment of lymphoma. We have studied Alemtuzumab in combination with EPOCH in this study

