

Introduction:
The preferred method for haploidentical stem cell transplantation (haploSCT) is currently the use of post-transplantation cyclophosphamide (PTCY) since it obviates the need for depletion of T lymphocytes, which is associated with profound immunosuppression. Despite preservation of non-alloreactive donor T cells, reconstitution of pathogen-specific immunity may be delayed even after T cell replete haploSCT. The incidence and clinical sequelae of viral reactivation may thus compromise the outcomes of the procedure.
Patients and Methods:
The study included 47 patients, who underwent haploSCT with PTCY from 12/2013 until 05/2019 and achieved stable donor engraftment. Median age at transplant was 53 years (range, 19-70). The indications for transplant were acute myeloid (n=19) or lymphoblastic (n=10) leukemia, myelodysplastic syndrome (n=10), myelofibrosis (n=4), chronic myeloid (n=2) or lymphocytic (n=1) leukemia, and T-prolymphocytic leukemia (n=1). Myeloablative conditioning was mainly utilized (n=36), with the exception of certain patients who received reduced-intensity (n=10) or non-myeloablative (n=1) regimens. The graft source was peripheral blood in 29 and bone marrow in 18 cases. Tacrolimus in combination with mycophenolate mofetil was administered for prevention of graft-versus-host disease. Recipient/donor cytomegalovirus (CMV) serostatus was -/- (n=2), -/+ (n= 5), +/- (n=11), or +/+ (n=29). CMV, Epstein-Barr virus (EBV), and human herpesvirus-6 (HHV-6) reactivation was monitored by real-time quantitative PCR (RQ-PCR) in plasma and/or leukocytes weekly for at least 6 months post haploSCT. BK virus (BKV) reactivation was assessed by RQ-PCR in urine and/or blood specimens in cases with symptoms suggestive of hemorrhagic cystitis (HC). Prophylaxis with letermovir was available in 1 patient only, and preemptive antiviral therapy was the principal modality for the management of CMV infection. Cellular immunity reconstitution was assessed by flow cytometry at 3, 6, and 12 months after transplant.
Results:
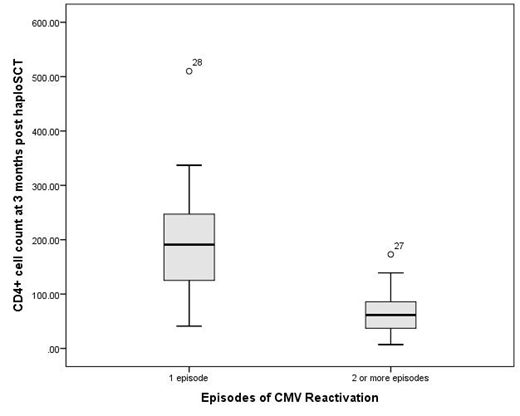
With a median follow-up time of 30 months (range, 2-64), the cumulative incidences (CIN) of relapse and non-relapse mortality (NRM) were 13.4% (95% confidence interval [CI], 5.4-25.1%) and 31.4% (95% CI, 18.3-45.4%) at 2 years, respectively. Disease-free (DFS) and overall survival (OS) were 55.2% (95% CI, 42.3-72.1%) and 61.8% (95% CI, 48.9-78.1%) at 2 years, respectively. The CIN of CMV reactivation (>100 copies/ml) plateaued at 75.6% (95% CI, 60.1-85.7%) at 3 months. CMV infection developed in 34 out of 45 patients who were at risk, whereas recurrent CMV reactivation was observed in 17 patients with a median number of 1.5 episodes (range, 1-6) per patient. The median total duration of antiviral therapy for CMV infection was 27 days (range, 14-199). CMV disease (pneumonia) was documented in 2 patients. The CIN of EBV reactivation (>1,000 copies/ml) was 47.1% (95% CI, 34.2-63.9%) at 12 months. No case of EBV-related post-transplant lymphoproliferative disorder was observed, however preemptive therapy with rituximab was required in 2 patients with rapidly increasing EBV viral load. HHV-6 reactivation (>1,000 copies/ml) was observed in 6 patients (CIN, 10.6% at 6 months; 95% CI, 3.8-21.4%), but only one required therapy with foscarnet due to high viral load (>10,000 copies/ml). The CIN of BKV-related HC reached 27.7% (95% CI, 15.7-40.9%) at 3 months. Cystoscopy for bladder hemostasis was required in 5/13 and nephrostomy in 1/11 patients with HC. Reconstitution of helper T cell immunity was considerably delayed, with median absolute CD4+ cell counts of 83/uL (range, 7-337), 216/uL (range, 80-509), and 236/uL (range, 97-586) at 3, 6 and 12 months, respectively. Recurrent CMV infection was significantly associated with the recovery of CD4+ cells at 3 months (Figure; median CD4+ count of 191/uL versus 62/uL in patients with 1 and 2 or more episodes of CMV reactivation, respectively; p=0.009).
Conclusions:
HaploSCT with PTCY is associated with substantial rates of viral reactivation (especially CMV and BKV) resulting in the need for prolonged antiviral therapy and considerable morbidity. Strategies to prevent viral infection are strongly warranted in haploidentical stem cell transplantation. The timing and duration of such interventions (like letermovir or adoptive immunotherapy) may be guided by the tempo of immune reconstitution following haploSCT.
Tsonis:Gilead: Other: Travel Grant; Astellas: Other: Travel Grants; Gilead: Other: Travel Grant; Aenorasis: Other: Travel Grant; Takeda: Other: Travel Grant; Pfizer: Other: Travel Grant; Innovis: Other: Travel Grant.

