

Introduction
'X-linked immunodeficiency with magnesium defect, Epstein-Barr virus (EBV) infection, and neoplasia' (XMEN) disease is a primary immunodeficiency disease caused by loss-of-function mutations in the MAGT1 gene encoding for the magnesium transporter 1. This leads to the absence of expression of the "Natural-Killer Group 2, member D" (NKG2D) receptor in natural killer (NK) and CD8+ T cells, which is essential for their antiviral and antitumoral cytotoxic activity. In consequence, XMEN patients develop chronic EBV infections and EBV-related lymphoproliferative disorders. Allogeneic bone marrow transplant has been associated with significant mortality, and there are no other effective treatments. In that context, we aimed at developing two complementary approaches to treat XMEN patients: 1) Adoptive transfer of XMEN T/NK cells corrected by transient mRNA therapy or longer-lasting gene editing therapy in order to control infections, and 2) Transplantation of gene-edited CD34+ cells in order to permanently restore production of functional immune cells.
Material and methods
CD34+ cells and PBMCs were collected from XMEN patients and healthy donors (HD) (NIH Protocol 94-I-073). For mRNA therapy, we expanded T cells with anti-CD3/anti-CD28 beads in RPMI + 10% serum supplemented with 200 IU/mL IL2 for 5-7 days and NK cells with 100 IU/mL IL2 and 10 ng/mL IL15 in culture with K562-mb15-41BBL for 10-15 days. Both XMEN T and NK cells were electroporated (EP) with MAGT1 mRNA and cultured for up to 28 days. For gene editing, XMEN CD34+ or stimulated T cells were electroporated with Cas9 mRNA and sgRNA; a rAAV6 donor encoding for the codon-optimized MAGT1 cDNA was added after EP. Two days post-EP, CD34+ cells were differentiated into NK cells for 35 days in vitro.
Results
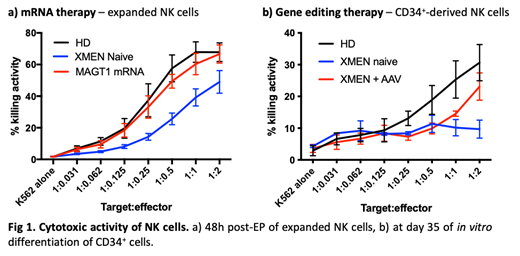
MAGT1 mRNA-based therapy. We first showed a restored MAGT1 expression by western blot at 6h and 24h post-EP of the MAGT1 mRNA. In consequence, NKG2D expression analyzed by flow cytometry was restored in expanded CD8+ T and NK cells starting within the 6h post-EP (20-40%), with a peak at 48h (>85%) and a progressive decrease of the expression over time (still 40% and 75%, respectively, of CD8+ T and NK cells of cells at day 14 post-EP respectively). The cytotoxic activity of mRNA-corrected XMEN NK cells was analyzed by culture with K562 target cells at several effector:target (E:T) ratios and shown to be restored at a level similar to HD NK cells (mRNA-treated: 66.7% ±5.8%; HD: 67.8% ±5.9% at E:T 2:1 ratio) compared to untreated cells (49.0% ±7.2%) (Fig 1a). Anticipating the potential use of these cells for repeated infusions as a treatment modality to control infections, we demonstrated that MAGT1 mRNA-corrected CD8+ T and NK cells that have been cryopreserved and thawed exhibit the same NKG2D expression kinetics following thaw and culture.
Gene editing therapy. XMEN CD34+ cells electroporated with Cas9 mRNA and a sgRNA targeting exon 1 of MAGT1 gene showed an in vitro average integration rate of the MAGT1 cDNA AAV donor of 35.6% (range: 33.8-41.9%). The NKG2D expression in AAV-treated CD34+-derived NK cells was approximatively of 23% (range: 14.2-27.9%). Interestingly, their cytotoxic activity was similar to the level of NKG2D expression (23.1% ±4.3%), significantly higher than in untreated cells (9.7% ±2.8%) (Fig 1b). Similar rates of targeted integration and NKG2D expression were also obtained in AAV-treated CD8+ T cells.
Conclusion
For the first time, we demonstrate the efficiency of two approaches for development of potential cell therapy treatments of XMEN patients. MAGT1 mRNA electroporation can restore efficient transient expression of NKG2D in CD8+ T and NK cells, thus fully restoring the cytotoxic activity of NK cells. In addition, cells electroporated with MAGT1 mRNA can be cryopreserved, thus allowing repeated infusions. In parallel, we showed that efficient targeted insertion can be achieved in CD8+ T cells and CD34+ cells by using an AAV donor although the level of NKG2D expression is lower. Optimizations are currently ongoing in order to reach higher levels of correction. Both approaches could be combined in order to propose a new therapeutic strategy for the treatment of XMEN patients: repetitive adoptive transfer of mRNA-corrected autologous T/NK cells for the prevention or control of intractable infections, and transplantation of gene-edited CD34+ cells for the definitive treatment of these patients.
Meis:CELLSCRIPT, LLC: Employment. Li:MaxCyte, Inc: Employment. Allen:MaxCyte, Inc: Employment. Clark:CELLSCRIPT, LLC: Employment. Dahl:CELLSCRIPT, LLC: Other: Owner and officer.

