

Background: Survival outcomes for multiple myeloma have improved dramatically since the introduction of novel therapeutic agents. While these drugs are highly effective in improving quantity and quality of life in patients with multiple myeloma, they are come at a significant financial cost. Cost effectiveness analysis is a commonly used tool to compare drug regimens to maximize value for health care dollars spent. The objective of this review is to assess the economic evidence for novel agents in the treatment of multiple myeloma.
Methods: A systematic literature review was conducted to assess the cost effectiveness and cost utility of novel agents in patients with multiple myeloma. The PRISMA checklist was followed. Medline (1946-present), EMBASE (1974-present), and Cochrane Database of Systematic Reviews (2005-present) were searched up to July 2019 for original publications that assessed the economic evidence for novel agents in multiple myeloma. Data was collected for all of the studies that met final inclusion criteria. The incremental cost effectiveness ratio (ICER) was the main outcome. Foreign currencies were converted to US dollars adjusted for inflation. The Quality of Health Economic Studies (QHES) checklist was used to assess study quality.
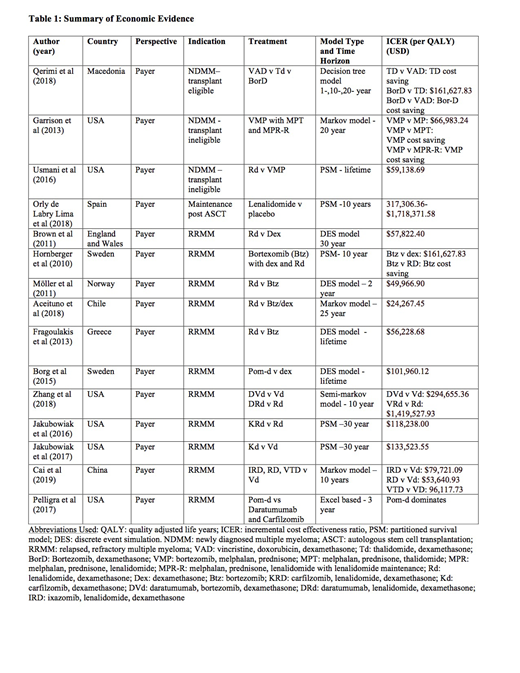
Results: The final search identified 279 records, however, 60 were duplicates. 219 articles were screened, however an additional 201 were excluded for the following reasons: did not meet inclusion criteria (100), systematic reviews or meta-analyses (9), letters to the editor (3), or conference abstracts (88). This left a remaining 19 abstracts for full text review, however full text was not available for 4 articles. Thus, 15 articles were included in the systematic review. Fifteen studies were identified involving novel agents (bortezomib, carfilzomib, thalidomide, lenalidomide, pomalidomide, ixazomib and daratumumab). Three studies assessed the cost effectiveness of novel agents in the frontline setting, 1 assessed the cost effectiveness of maintenance following autologous stem cell transplantation, and the remaining 9 assessed novel agents in the relapsed setting. There was significant heterogeneity in the national perspective of the assessments with the majority being from a payer's perspective in the United States. Economic models varied considerably between the studies with the majority being one of: a partitioned survival analysis, Markov model or discrete event simulation. The time horizon for the models varied between 2 years and a lifetime with the majority being 10 years or longer. Economic evidence was of at least fair quality as assessed by the QHES checklist. The results of the economic analyses are summarized in Table 1. In general, novel agents were considered cost effective when used in both the frontline and relapsed setting. They were cost effective when compared to both steroids and traditional cytotoxic chemotherapy. While combinations of novel agents are clinically effective, cost effectiveness was dependent on individual drug prices as well as one's willingness to pay threshold. The main factors that influence the incremental cost-effectiveness ratio are survival outcomes and drug price.
Discussions and Conclusions: This review highlights the need for ongoing research into cost effectiveness of novel agents in multiple myeloma. In general, novel agents are considered cost effective, however; there were a relatively small number of papers ion this topic and conclusions should be drawn with caution regarding the cost effectiveness of specific agents and regimens. Additionally, the studies in this review were quite heterogeneous in terms of the country of analysis, economic model, and study population, which will also influence their generalizability. As well, economic analyses of the same drug regimens showed significant variability, as was the case of lenalidomide maintenance, dependent on data inputs used. Further, the majority of these studies relied on list price for their cost inputs into the model, thus the actual cost effectiveness of a treatment regimen will depend on the final, negotiated drug price, which is often significantly less. Finally, as these models do not account for other factors, such as sequencing and patient and provider preferences, caution must be used when using economic analysis as the sole factor in guiding decision making.
McCulloch:Celgene: Honoraria; Amgen: Honoraria.

