

Background: Thrombotic Thrombocytopenic Purpura (TTP) is a form of microangiopathic hemolytic anemia that is classically characterized by the clinical pentad of fever, hemolytic anemia, thrombocytopenia, renal dysfunction, and neurologic dysfunction. The pathophysiology of acquired TTP is marked by autoantibody formation against ADAMSTS13, an enzyme responsible for breaking down von Willebrand Factor (vWF) multimers. Standard therapy for TTP includes both replenishing functional ADAMTS-13 and immune-modulation with plasma-exchange and steroids/rituximab, respectively. A novel therapy addresses the microvascular thrombosis hallmark of end-organ damage in TTP. Caplacizumab, a humanized immune globulin that inhibits vWF interaction with platelets, achieved its primary endpoint of faster time to platelet normalization than placebo in the Stage 3 HERCULES trial when given up-front with additional standard therapies.
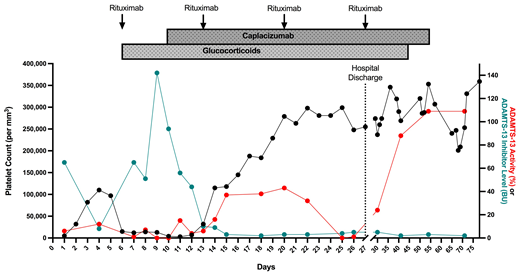
Case Summary: A previously health 26-year-old G3P2 female presented to the ED at 38 weeks gestation with fatigue and confusion. She was found to have a platelet count of 5,000 per microliter, hematocrit of 18.6%, lactate dehydrogenase (LDH) of 1,750 IU/L, and haptoglobin of 11mg/dL. Peripheral blood smear was remarkable for evidence of microangiopathic hemolytic anemia. She had a normal serum creatinine. She was diagnosed clinically with TTP and subsequently underwent emergent caesarian section. She was started on plasma exchange given her ADAMTS13 activity of 6% and features of severe TTP. Her neurological status and platelets initially responded well to plasmapheresis (PE) at 1x volume alone; however, on Day 6 her platelets decreased from 97,000 to 15,000 per microliter. This prompted initiation of both steroids, weekly rituximab and increasing PE to 1.5 x. She continued to be refractory and acutely declined on Day 7, during which she developed worsening headaches followed by seizure, renal failure with proteinuria, uncontrolled hypertension and increasing hemolysis. She required ICU admission and one session of hemodialysis. Despite increasing PE, steroids and rituxan, the patient's inhibitor peaked to 142 U/ml with an ADAMTS-13 activity of 0% on Day 9. PE was increased to 1.5 x volume twice daily. Caplacizumab was obtained and initiated on Day 10. Her platelets on Day 11 were at their nadir of 4,000 per microliter, with an inhibitor of 93.9 and an ADAMTS-13 activity of 0%. She remained in the ICU, where her mental status, renal function improved gradually. She was found with a reticulocyte index of 1.29, for which she was treated with Vitamin B-12 for a methylmalonic acid level of 798 nmol/L (range 87-318 nmol/L) and a low normal level of vitamin B-12. PE was stopped on Day 22 after confirming her platelet level remained >150,000 per microliter for more than three days. Her course was further complicated by aspiration, parainfluenza 3, MSSA bacteremia, and E Coli UTI, for which she received antibiotics and supportive treatment. She completed four cycles of rituximab on Day 27, and was discharged to home with a steroid taper and an additional 21 days of caplacizumab. She was readmitted three times during those 21 days for hemiplegic migraines. She achieved remission with normal complete blood count and ADAMTS13 >109% with an inhibitor 3 on Day 54, after which she was administered her last dose of caplacizumab on Day 56. Discussion: We detail the clinical and treatment course in our patient with severe, acquired TTP from pregnancy. Our timing of caplacizumab administration differed from that in the HERCULES Trial. Rather than administering caplacizumab at the onset of diagnosis, we utilized markers of end-organ damage, ADAMTS13 activity and inhibitor level to gauge the trajectory of the disease process before administering additional therapies. This may represent an alternative approach to treating aTTP in a post-caesarian patient given concern for risk of bleeding and lack of trial data that adequately captures the bleeding risk of this sub-population. Lastly, we describe reticulocytopenia and Vitamin B12 deficiency in this patient complicating her recovery from TTP. The etiology of her B12 deficiency is still unclear ( anti-parietal antibody titer <1:120).
No relevant conflicts of interest to declare.

