

INTRODUCTION: Human cytomegalovirus (HCMV) infection is a significant cause of mortality and morbidity after hemopoietic stem cell transplantation (HSCT). Pre-emptive therapy with Ganciclovir (GCV) reduces the risk for HCMV disease but may be associated with significant toxicity. Letermovir (LTV) has been recently approved for prophylaxis of HCMV infection in HCMV-seropositive patients.
AIM: to compare costs associated with GCV preemptive therapy or LTV prophylaxis within 100 days after HSCT.
METHODS: A retrospective analysis of GCV preemptive therapy-related costs was performed on 63 HCMV-seropositive patients receiving allogeneic HSCT. For comparison, we estimated LTV prophylaxis-related costs according to dosage and duration reported in the phase 3 trial (Marty et al., NEJM 2017). According to definitions adopted in the LTV prophylaxis study, patients were considered at high risk for HCMV-disease if having one of the following: a mismatched (related or unrelated) or a haploidentical donor; umbilical cord blood as the stem-cell source; ex vivo T-cell-depleted grafts; and grade ≥2 GVHD. Clinically significant HCMV infection was defined as HCMV disease (i.e. HCMV end-organ infection in association with clinical symptoms) or HCMV DNAemia leading to pre-emptive treatment (i.e. ≥ 30.000 copies/mL in blood in the GCV-preemptive group; ≥ 150 copies/mL or ≥ 300 copies/mL in plasma for high-risk or low-risk patients in the LTV-prophylaxis study). All diagnostic and therapeutic procedures performed within 100 days post-HSCT were recorded. Costs associated to HCMV antiviral therapy and to the management HCMV infection (including also, but not limited to, diagnostic procedures, transfusions and hospitalizations) were calculated.
RESULTS
Study populations
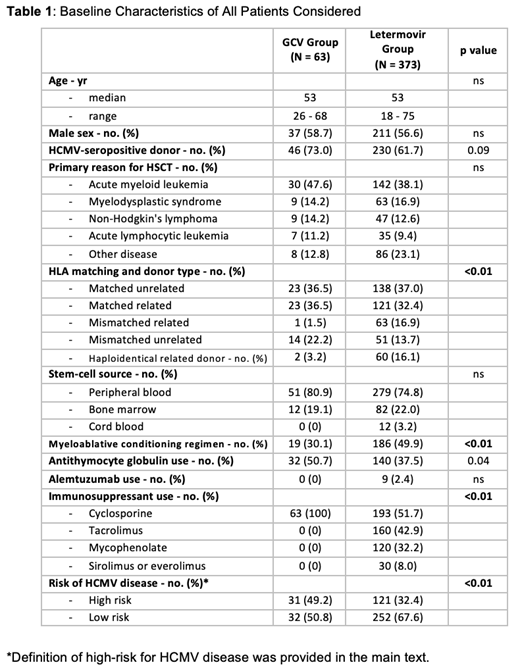
Baseline characteristics of the GCV-preemptive group in comparison with the LTV-prophylaxis group are shown in Table 1. A higher proportion of patients at high risk for HCMV disease has been observed in the preemptive group (49.2% vs 32.4%).
HCMV infection and disease
GCV-preemptive group: 39 patients (62%) developed a clinically significant HCMV infection and in all cases pre-emptive therapy resolved the infection. Drug switch due to GCV-induced neutropenia was not necessary in any case. Gastrointestinal HCMV disease occurred beyond day 100: in 2 patients (3.2%) occurred within 24 weeks post-HSCT and in additional 7 patients later on (median time: 314, range 144-387 days after HSCT).
LTV-prophylaxis group: clinically significant HCMV infection occurred in 57/325 (17.5%) patients with 5 (1.5%) developing gastrointestinal HCMV disease within 24 weeks after HSCT. Data for HCMV disease beyond week 24 are not reported.
Costs analysis
GCV-preemptive group: 5 mg/kg GCV has been administered i.v. twice daily. One vial of GCV 500 mg is purchased at a cost of 57.67 €. The average duration of GCV therapy was 16.9 days and the average cost was 77 €/day, i.e. 1301.67 €/patient. Six patients (10%) were hospitalized for the management of HCMV infection, for a total cost of 22,428 € (356 €/patient). Thus, the overall cost was 1657.67 €/patient (78% directly related to GCV-therapy and 22% related to the healthcare management costs).
LTV-prophylaxis group: 240 mg/day of oral LTV were administered for of 100 days. Twenty-eight tablets of LTV cost of 13,863.36 €. Thus the total cost for LTV administration is 49,512 €/patient (or 24,756 € for patients receiving cyclosporine). We did not consider costs associated to HCMV reactivation. The costs for HCMV management with LTV prophylaxis appears to be ≥15 times superior to the costs for GCV preemptive therapy
CONCLUSIONS: LTV prophylaxis is effective in reducing the risk for HCMV disease. However, the costs are superior to those for GCV-preemptive therapy (also considering hospitalization costs). Prospective randomized studies are needed to compare directly different outcomes in HSCT recipients receiving LTV prophylaxis vs GCV preemptive therapy (such as overall costs, indirect effects of subclinical HCMV infection, overall patient's survival). Nevertheless, the identification of patients at lower risk for HCMV infection (thus not requiring prophylaxis), as well as a personalized administration of LTV prophylaxis on the basis of the individual time to immune reconstitution (thus tailoring duration of prophylaxis), will be of great help for sparing costs in Health Systems with limited resources.
No relevant conflicts of interest to declare.

