

Introduction: Non-myeloablative conditioning regimens enable elderly and younger patients with significant comorbidities to undergo allogenic stem cell transplant (allo SCT). These regimens allow for the benefit of graft-versus-leukemia (GVL) effect with reduced toxicity. A retrospective analysis of 94 patients with acute myeloid leukemia (AML) who received a non-myeloablative transplant with fludarabine (25 mg/m2 days -7 through -3)/cyclophosphamide (1000 mg/m2 days -7 and -6) (Flu/Cy) conditioning was conducted to evaluate patient outcomes.
Methods: Ninety-four patients with AML underwent non-myeloablative allo SCT with Flu/Cy conditioning at Penn State Cancer Institute between 2007 and 2015 were retrospectively analyzed. The patients were deemed ineligible for myeloablative or reduced intensity conditioning transplants due to advanced age or significant comorbidities. Most unrelated donor patients (n=69) received tacrolimus/sirolimus/methotrexate as graft-versus-host disease (GVHD) prophylaxis. Overall survival (OS) and disease-free survival (DFS) were assessed with Kaplan-Meier survival curves and log rank tests, and non-relapse mortality (NRM) and relapse rates (RR) were assessed with cumulative incidence of competing events and Gray test. Cox proportional hazard regression with stepwise selection was used for multivariate analysis.
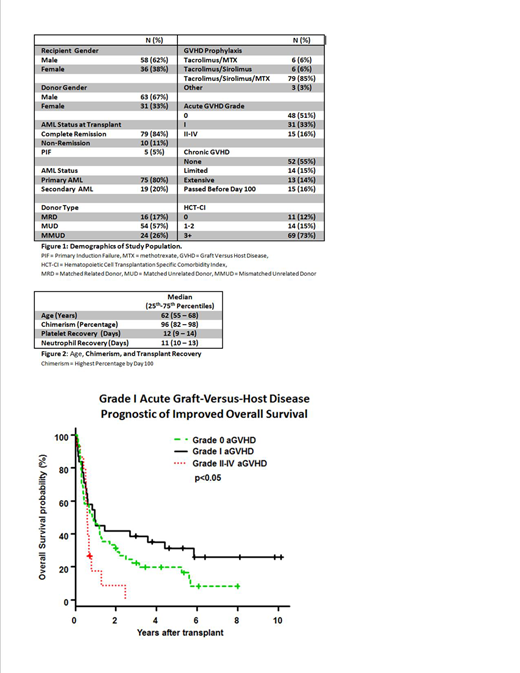
Results: Patients with AML underwent Flu/Cy conditioning for allo SCT from either a matched related donor (MRD) (n =16), matched unrelated donor (MUD) (n=54), or mismatched unrelated donor (MMUD) (n=24). Evaluation of AML status immediately prior to allo SCT identified 79 patients in complete remission, 10 patients with non-remission, and 5 patients with primary induction failure. There were 11 patients with hematopoietic cell transplantation specific comorbidity index (HCT-CI): 0, 14 patients with HCT-CI: 1-2, and 69 patients with HCT-CI: ≥3. Post-transplant analysis identified: 48 patients with grade 0, 31 patients with grade I, and 15 patients with grade II-IV acute graft-versus-host disease (aGVHD). Furthermore, 52 patients were without chronic GVHD (cGVHD), 15 experienced limited cGVHD, and 13 experienced extensive cGVHD. One-year OS and DFS were 41.3% (95% CI: 31.3-51%) and 27.7% (95% CI: 18.7-37.4%), respectively. One-year NRM and RR were 12.9% (95% CI: 0.68-21%) and 59.5% (95% CI: 48.2-69.1%). There were no statistically significant differences in NRM between patients with varying comorbidity indices. One-year OS for patients in complete remission versus non-remission prior to transplant was 45.3% versus 20.0% (p<0.01), and was significantly greater in patients with grade I versus grade II-IV aGVHD (45.2% versus 17.8%, p<0.05). Patients with cGVHD showed a lower RR compared to patients without cGVHD (1-year RR 20.4% vs 48.5%, p<0.05). Patients who achieve a chimerism ≥90% within 100 days of transplant achieved a better OS and lower RR compared to patients with a chimerism <90% (1-year OS 51.3% versus 21.4%, p<0.01; 1-year RR 44.0% vs 89.3%, p<0.01, respectively). Multivariate analysis identified grade I aGVHD (versus grade II-IV, p<0.01), cGVHD (versus no cGVHD, p<0.05), and chimerism ≥90% (versus <90%, p<0.05) as independent factors for improved OS.
Conclusions: The primary endpoint for this retrospective analysis was OS following non-myeloablative allo SCT for AML utilizing Flu/Cy conditioning. Although RR was high (59.5%), this conditioning regimen resulted in rapid stem cell recovery and low NRM. There were no significant differences in NRM between patients with lower (0, or 1-2) and higher (≥3) HCT-CI and patients receiving MRD, MUD or MMUD. This confirms that Flu/Cy conditioning is safe, especially for patients with multiple comorbidities and receiving MMUD. This analysis also identified a significant improvement in OS for patients with grade I as compared to grade II-IV aGVHD. Also, patients with cGVHD showed a significantly reduced RR. Collectively, the improved survival for patients with grade I aGVHD and cGVHD may be associated with a more robust GVL effect. Additionally, patients who achieve a higher chimerism showed a reduced RR. This study highlights the tolerability of Flu/Cy and the importance of balancing GVHD and GVL effects; future studies are needed to evaluate the addition of maintenance therapies to overcome higher RR occurring with this regimen.
Naik:Celgene: Other: Advisory board. Zheng:Pfizer: Research Funding. Claxton:Daiichi Sankyo Co. and Ambit Biosciences Corp, Astellas Pharma, Novartis Pharmaceuticals, Incyte Corporation, Cyclacel Pharmaceuticals, Inc, Celegene Corporation, Medimmune, Inc, Merck Sharp & Dohme Corp., Gilead Sciences, Inc.: Research Funding.

