

Brain death is a permanent loss of all brain function [1]. Current clinical organ transplantations mostly depend on the organs from brain-dead patients [2]. And of note, a lot of blood deases are easy to cause cerebral haemorrhage, which is quite of danger and usually induce brain death if not detected and treated in time. Thus prompt evaluation of brain death is of great significance for saving medical resources and reducing economic burden of the patients' families. Current guide for diagnosing brain death required to perform a list of >30 hours neurological examninations, some of which are even invasive, not in time and easily hampered by many confounding factors. An ideal ancillary test to assess brain death is highlighted to be noninvasive, sensitive, universally available, timely, and easy to perform at the bedside. Near infrared spectroscopy ( NIRS ) is capable of monitoring hemodynamics in response to brain activity noninvasively, conveniently, continually, and relatively inexpensively, evidented by a series of clinical cerebral studies recently. Weigl et al newly reported to use a time resolved NIRS to detect the fluorescence photons excited in the indocyanine green ( ICG ) for cerebral perfusion detection. It provided a novel optical ancillary tool to assess brain death, while its accuracy was only 69.2%, which did not reach the level of brain death confirmation. Plus, it was invasive, requiring injection of optical contrast agent.
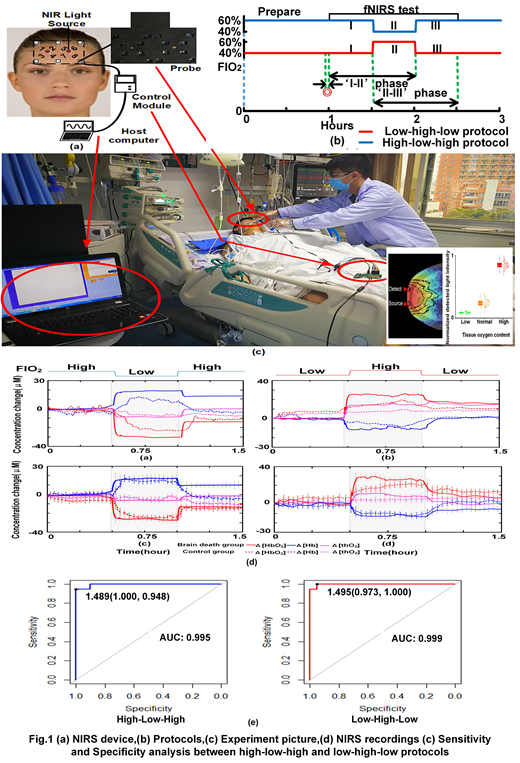
We attempted to assess brain death completely in nonivasive way with just a custom wearable NIRS device developed in our lab [3] ( fig.1 a ). We novelly incororate a protocol at markedly but safely varied fractions of oxygen respiration. Firstly, Monte Carlo modeling were carried out to test the difference in photon transport within human brain at different oxygen concentrations induced by varied fractions of oxygen respiration ( FIO2 ) [4]. 18 healthy subjects ( 41 ± 11 years old ) and 17 brain dead patients were recruited from the intensive care unit (ICU) in Sichuan Academy of Medical Sciences & Sichuan Provincial People's Hospital. No significant difference in age was found between patients and healthy groups ( p >0.413 ). These patients were finally clinically diagnosed by the international standards of brain death. Two protocols were used ( fig.1 b). One is consisted of 1 hour resting, 3-minute baseline measure, half-hour measurement at 60% FIO2 ( phase I, high oxygen ),a half hour measure at 40% FIO2 ( phase II, low oxygen ), and a half hour measure at 60% FIO2 ( phase III, high oxygen ). The other is low, high, and low. The Δ[Hb] and Δ[HbO2] time courses were recorded by NIRS in real time with related signal processing ( fig.1 c ). Statistical analysis were focus on the sensitivity and specificiy of our proposed methodology at combination of NIRS and above protocol, as well as which protocol act better.
Fig.1 ( c right ) showed that the detected light signal profile dramatically differed among varied oxygen concentrations in human brain. Plus the hemodynamic responses varied clearly between two subject groups among varied FIO2 in both protocols ( fig1. d ). The ' II-III ' phase act more distinct in differing two groups than ' I-II ' phase. And the low-high-low protocol acted almost perfect in accessing brain death with highest sensitivity and specificity.
Over all, the novel incorporation of NIRS and a low-high-low varied FIO2 protocol was shown to a be most sensitive, highly specific, noninvasive and real time way to assess brain death and promptly offer quality assured donor organs.
[1] E. F. M. Wijdicks, P. N. Varelas, G. S. Gronseth, D. M. Greer, Evidence-based guideline update: Determining brain death in adults report of the quality standards subcommittee of the American Academy of Neurology, Neurology, vol. 74, no. 23, pp. 1911-1918, 2010
[2] K. Singbartl, R. Murugan, A. M. Kaynar, D. W. Crippen, S. A. Tisherman, K. Shutterly, S. A. Stuart, R. Simmons, Intensivist-led management of brain-dead donors is associated with an increase in organ recovery for transplantation, J. M. Darby, Am. J. Transplant., vol. 11, no. 7, pp. 1517-1521, 2011
[3] T. Li, M. Duan, Y. Zhao, G. Yu, Z. Ruan. Bedside monitoring of patients with shock using a portable spatially-resolved near-infrared spectroscopy. Biomed. Opt. Express, vol. 6, no. 9, pp. 3431-3436, 2015
[4] B. Pan, C. Huang, X. Fang, X. Huang, T. Li*, Noninvasive and Sensitive Optical Assessment of Brain Death, J. Biophotonics, vol. 12, no. 3, pp. e201800240, 2018
No relevant conflicts of interest to declare.

