


Targeted agents have greatly improved outcomes for patients (pts) with chronic lymphocytic leukemia (CLL) and other B cell lymphomas; however, single agents have been limited by intolerance, resistance and depth/durability of responses. Current novel targeted agent combinations may improve depth of response, but such "full dose" strategies have been associated with significant AEs, dose reductions/interruptions and discontinuations.
Our in vitro & in vivo screening/optimization studies identified that concurrent inhibition of BTK & mTOR targets plus IMiD at low doses of each inhibitor can synergistically kill B-cell malignancies and may address drug-resistance. DTRM-555 is an optimized oral triplet combination of a novel BTK inhibitor DTRMWXHS-12 (DTRM-12) with everolimus (EV) & pomalidomide (POM). This once daily therapy was tested in a stepwise, phase I, US multicenter study in patients with highest unmet medical needs including r/r CLL, Richter's transformation (RT) of CLL, DLBCL, transformed B-cell lymphomas.
We conducted a 3+3 design phase I, first human trial exploring DTRM-555 in pts ≥18 years, ECOG PS ≤1 with CLL, B-cell NHL, or Hodgkin lymphoma (HL) with no available standard therapy (NCT02900716). Our goal was to determine optimal doses for triplet combination therapy through 3 escalating phases of study: DTRM-12 in escalating doses (50, 100, 200, & 300 mg/day) in Part Ia, DTRM-12 at 200 mg or 300 mg & EV at 5 mg (doublet or DTRM-505) in Part Ib Arm A while DTRM-12 at 200 mg or 300 mg, EV at 5 mg & POM at 2 mg in Part Ib Arm B. For all arms, treatment was administered for 21 consecutive days of a 28-day cycle, until disease progression or unacceptable toxicity. Safety was the primary endpoint, and the dose-limiting toxicity (DLT) period was cycle 1. Secondary endpoints included response (iwCLL 2018 or Cheson 2014), progression free survival, duration of response and pharmacokinetics. Intra-patient migration between arms (Mono to doublet to triplet) was permitted if subsequent doses were tolerated. The trial commenced 9/27/2016 and completed enrollment 7/25/2019.
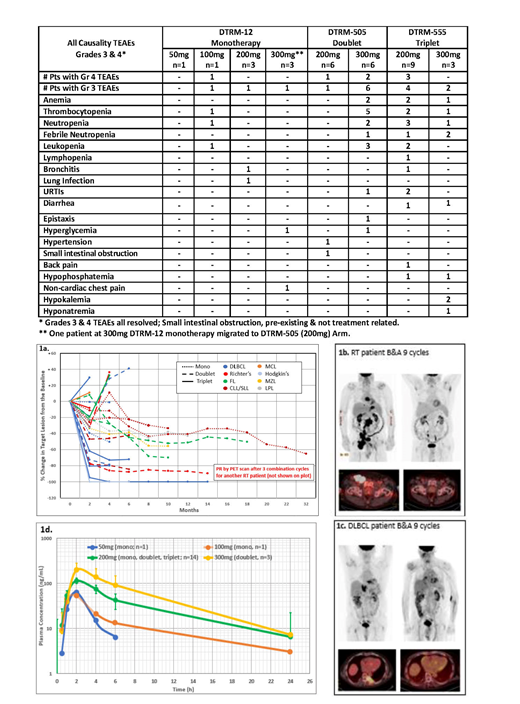
Thirty-three pts were enrolled, including 2 screen failures and 4 intra-cohort migrations, with r/r DLBCL (n=8), CLL/SLL (n=5), RT (n=6), FL (n=5), MCL (n=4), MZL/LPL (n=3), HL (n=2). 30 of 31 treated pts were evaluated: 8 pts participated in phase Ia (DTRM-12) while 23 pts were treated on phase Ib combinations (DTRM-505 & DTRM-555). Baseline characteristics: 70% male (n=23), median age 70 years (range 46-94) and 94% white. Median prior therapies were 3 (range 1-10), 53% had been treated with ≥1 prior targeted agent (i.e., CD19/CD3 bispecific antibody, obtinutuzumab, pembrolizumab, nivolumab, ibrutinib, venetoclax, PI3k-i), CAR-T or HSCT. 35% pts were previously treated with ibrutinib. Table 1 describes Grade (Gr) 3 and 4 AEs (all causality, stratified by treatment arm). Regarding safety, AEs were manageable, with a total of 5 DLTs were observed: 2 (Gr 3 febrile neutropenia, URI) in part Ib arm A, 3 (Gr 4 thrombocytopenia, Gr 3 diarrhea, G3 febrile neutropenia) in Part Ib arm B. No MTD was reached for the mono & doublet arms, with the MTD of the triplet determined to be DTRM-12 200 mg, EV 5 mg, & POM 2 mg. Spider plot (Figure 1a) shows the clinical response for individual CLL and lymphoma pts treated with mono, doublet and triplet therapies. Depth and durability of response improved with combination therapies (vs. mono). Of note, 48% of all patients had a ≥50% reduction in sum of the products of lymph node diameters. Representative PET-CT scans are in Figure 1b-c. Responses in multi-refractory pts are ongoing (including 15+ mos in a pt with r/r DLBCL and 5+ mos PR in a pt aged > 90 yrs with r/r DLBCL; 4+ & 13+ mos PRs in two pts with RT). DTRM-12 plasma concentrations were unaffected by EV & POM (Once Daily Oral Therapies) in Figure 1d.
The clinical trial met its primary endpoint as the triple combination DTRM-555 had an acceptable safety profile. Dose dependent drug levels with minimal inter-pt variations were observed in all arms, supporting once daily oral administration of this low-dose combination therapy. Encouraging clinical activity was observed in several high-risk, multi-refractory CLL and lymphoma pts, including those previously treated with ibrutinib. Thus synthetic lethality is a viable treatment approach. A phase II US expansion study is underway targeting pts with transformed lymphomas (follicular or prior CLL) and r/r DLBCL cohorts.
Mato:AbbVie: Consultancy, Research Funding; Sunesis: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; Johnson & Johnson: Consultancy, Research Funding; Celgene: Consultancy; AstraZeneca: Consultancy, Research Funding; Pharmacyclics: Consultancy, Research Funding; Gilead: Research Funding; Acerta: Consultancy; Janssen: Consultancy; TG Therapeutics: Consultancy, Other: DSMB member , Research Funding; LOXO: Consultancy, Research Funding; DTRM Biopharma: Research Funding. Schuster:DTRM Biopharma: Research Funding. Foss:Mallinckrodt: Consultancy; Acrotech: Consultancy; miRagen: Consultancy; Seattle Genetics: Consultancy, Other: fees for non-CME/CE services ; Eisai: Consultancy; Spectrum: Other: fees for non-CME/CE services . Isufi:Novartis: Consultancy; Astra Zeneca: Consultancy; Celgene: Consultancy. Ding:Merck: Research Funding; DTRM Biopharma: Research Funding. Brander:Novartis: Consultancy; MEI: Research Funding; Pharmacyclics LLC, an AbbVie Company: Consultancy; BeiGene: Research Funding; AstraZeneca: Consultancy, Research Funding; Acerta: Research Funding; Tolero: Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Genentech: Consultancy, Honoraria, Research Funding; Teva: Consultancy, Honoraria; TG Therapeutics: Consultancy, Honoraria, Research Funding; DTRM Biopharma: Research Funding. Tun:Mundi-pharma: Research Funding; TG Therapeutics: Research Funding; Curis: Research Funding; DTRM Biopharma: Research Funding; Celgene: Research Funding; BMS: Research Funding. He:DTRM Biopharma: Employment, Equity Ownership. Kearney:DTRM Biopharma: Employment, Equity Ownership. Gui:DTRM Biopharma: Employment, Equity Ownership. Anderson:Theradex: Employment. Roeker:AbbVie: Equity Ownership; Abbott Laboratories: Equity Ownership. Huntington:Bayer: Consultancy, Honoraria; AbbVie: Consultancy; Celgene: Consultancy, Research Funding; Genentech: Consultancy; Pharmacyclics: Honoraria; DTRM Biopharm: Research Funding.
Everolimus in B cell lymphomas and CLL Pomalidomide in B cell lymphomas and CLL
This icon denotes a clinically relevant abstract

