


Background: The prognosis for patients (pts) with relapsed T-ALL and T-LL is dismal; the primary goal of T-ALL/T-LL treatment is to prevent relapse. AALL1231 was a COG phase 3 clinical trial that randomized children and young adults (age 1-30 years) to a modified augmented BFM (aBFM) backbone +/- the proteasome inhibitor bortezomib during induction and delayed intensification (DI) (1.3mg/m2 x 4 doses per block). Bortezomib was tested in frontline therapy based on strong preclinical data and data in relapse on COG AALL07P1. Pts were stratified as standard (SR), intermediate (IR), or very high risk (VHR), primarily based on disease response: morphologic and minimal residual disease (MRD) at end induction and end consolidation (T-ALL) and radiographic response (T-LL). To eliminate cranial radiation (CXRT) in all pts, (except VHR: Day 29 M3 marrow or EOC MRD >0.1% or pts with overt CNS leukemia at diagnosis, CNS3), the aBFM backbone was modified to use dexamethasone (dex) as the sole corticosteroid and an extra pegaspargase dose was added in both induction and DI, following the MRC strategy. IR pts received a second interim maintenance (IM) phase (one Capizzi MTX; one HD-MTX). Following consolidation, VHR pts received 3 BFM high-risk intensification blocks in lieu of IM.
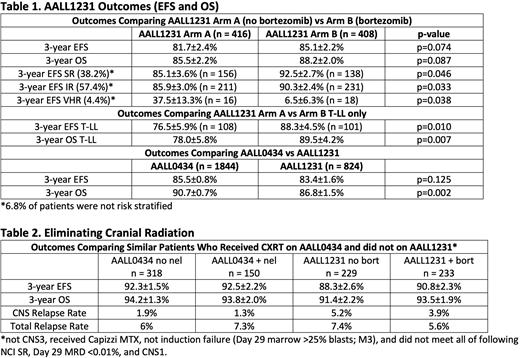
Results: AALL1231 accrued 847 patients (824 eligible and evaluable) of 1400 anticipated from 2014 until early closure in 2017 when COG AALL0434 established that nelarabine (NEL) improved DFS in T-ALL (AALL1231 did not include NEL). The 3-year EFS for Arm A (no bortezomib) vs Arm B (bortezomib) were 81.7±2.4% and 85.1±2.2 % (HR=0.782, p=0.074) (3/31/20 data cut-off; see Table 1 for additional outcomes). SR and IR pts, who account for 95% of pts, had significantly improved EFS on Arm B as compared with Arm A. Yet, VHR patients had improved EFS on Arm A. Patients with T-LL had improved EFS and OS with bortezomib: 3-year EFS (76.5±5.9% vs 88.3±4.5%; p = 0.01); 3-year OS (78.0±5.8% vs 89.5±4.2%, p = 0.007). A similar improvement in EFS and OS was not seen in T-ALL; however, with longer follow-up this may change. No excess toxicity was seen on Arm B.
A dex-based Induction did result in lower MRD rates; more T-ALL pts on AALL1231 had Day 29 MRD <0.1% as compared with AALL0434 which used a prednisone-based Induction (AALL1231 Arm A: 69.6%; Arm B: 72.2%; AALL0434: 64.6%; p = 0.02). However, this did not translate into improved survival. Indeed OS, but not EFS was worse on AALL1231 than AALL0434. On-going analyses are investigating the increased mortality on AALL1231, but preliminary analyses suggest a combination of increased toxic deaths and overall poor outcome in the VHR group.
On AALL0434, 90.8% of T-ALL pts received CXRT. On AALL1231, 9.5% of subjects were scheduled to receive CXRT (CNS3 T-ALL/T-LL: 5.7%; VHR T-ALL: 4.1%). A comparison of AALL0434 pts that received CXRT with similar AALL1231 pts not receiving CXRT on AALL1231 demonstrated similar EFS (p = 0.14) and OS (p = 0.42) (Table 2). CNS relapse rates were higher in these pts on AALL1231 (4.5%) as compared with AALL0434 (1.7%), but overall relapse rates were the same (6.5% vs 6.4%). Notably the benefit of NEL in AALL0434 was due to reduction of CNS relapses. 128 AALL1231 pts came off protocol therapy after the study was closed for physician or patient/parent choice. Data collection is underway to understand the reasons for removal, including if it was to receive NEL.
Conclusions: Outcomes for SR and IR pts with T-ALL and T-LL treated with bortezomib were excellent despite the elimination of prophylactic CXRT. Bortezomib significantly improved 3-year EFS for these groups, comprising ~95% of pts. Outcomes for VHR pts were dismal and worse on the bortezomib arm. T-LL pts had significantly improved EFS and OS with bortezomib on the AALL1231 backbone. This is the first trial to demonstrate an OS benefit for de novo pediatric T-LL with a new agent; however, longer follow-up is needed. Therapy intensification allowed elimination of CXRT in the majority of pts without excessive relapse. These results should be interpreted cautiously as the 3-yr OS on AALL1231 was inferior to AALL0434. Nevertheless, incorporating bortezomib into standard therapy for de novo T-LL appears advantageous. Future COG T-ALL/T-LLy trials will build on the positive findings from AALL0434 and AALL1231, balancing intensity while mitigating toxicity to maintain high cure rates without routine cranial radiation. (MLL, SPH, EAR contributed equally)
Teachey:Amgen: Consultancy; Janssen: Consultancy; La Roche: Consultancy; Sobi: Consultancy. Dunsmore:Dexcom: Current equity holder in publicly-traded company. Galardy:Abbott: Current equity holder in publicly-traded company; Abbvie: Current equity holder in publicly-traded company. Harker-Murray:Regerenon Pharmaceuticals: Consultancy. Hermiston:Sobi: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees. Shimano:Novartis: Research Funding; Daiichi Sankyo: Research Funding; Pfizer: Research Funding; Dova Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees. McKay:Immunogen: Current Employment. Bollard:Mana Therapeutics: Other: IP. Loh:Medisix Therapeutics: Membership on an entity's Board of Directors or advisory committees; Pfizer: Other: Institutional Research Funding. Hunger:Novartis: Consultancy; Amgen Inc.: Current equity holder in publicly-traded company, Honoraria. Raetz:Celgene/BMS: Other; Pfizer: Research Funding.
Bortezomib for the treatment of acute lymphoblastic leukemia under an IND
This icon denotes a clinically relevant abstract

