

Background: AML is a heterogeneous hematological cancer, characterized by the clonal expansion of myeloid blasts in the peripheral blood, bone marrow and other tissues. Among adults, AML is the leading cause of leukemia-associated death. Patients are often elderly and have comorbid conditions. Response to remission induction therapy varies by biologic subtype and by the drugs used for induction, but responses to each therapy are not predictable, even within specific biologic subgroups. To improve prognostication and identify new therapeutic options, Cellworks developed the Cellworks Omics Biology Model (CBM) that relies on multi-omics inputs from malignant cells to predict response and identify potential therapies tailored to the unique mechanisms of each patient's disease.
Aim: To predict the response to induction chemotherapy regimens in AML patients and identify predictive genomic signatures, pathways, and personalized treatment options for refractory patients.
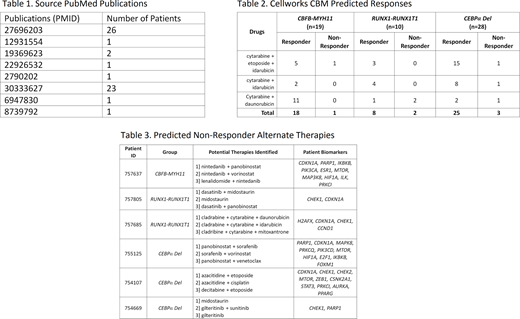
Method: 57 AML patients with known therapy response were selected from 8 PubMed publications (Table 1). The cohort was split into 3 groups with CBFB-MYH11 fusion (n=19), RUNX1-RUNX1T1 fusion (n=10) and CEBPα del (n=28). All data was anonymized, de-identified and exempt from IRB review. NCCN offers specific recommendations for AML patients with these mutations and they are associated with high rates of remission after induction therapy. The available genomic data for each profile was processed using Cellworks' CBM to generate an AML subtype-specific protein network map using published information from PubMed and other online resources permitting patient-specific biomarkers to be mapped to sensitivity and resistance pathways. Drugs selected from a digital drug library were simulated for each patient across the three cohorts. Benefit was assessed by measuring each drug's effect on a cell growth score, a composite of proliferation, viability, and apoptosis indices.
Results: Of 57 patients with favorable-risk AML, 6 (11%) experienced induction failure. 1/19 patients harboring CBFB-MYH11 fusion failed to respond to induction therapy (Table 2) and CBM identified co-occurring gene aberrations responsible for resistance in the patient with resistant disease (ID:757637), who harbored trisomy 6 with amplification of GSTA1, GSTA2, GSTA4, DEK, TFAP2A, NFYA and EHMT2 causing dysregulation of pathways involved in treatment failure. CBM also identified 3 prospective therapies that target this patient's specific biomarkers (Table 3).
Similarly, 2/10 patients with RUNX1-RUNX1T1 fusion failed to respond to induction therapy. CBM identified a loss of function mutation in EZH2 causing increased levels of HOXA5 and HOXA9 as key orchestrators of treatment failure (Patient ID: 757805). Furthermore, CBM also identified 3 prospective therapies for this patient, targeting patient-specific resistance mechanisms (Table 3).
In the CEBPα cohort, 3/28 patients did not respond to induction therapy (Table 2). For Patient ID:755125, CBM identified a DNMT3A loss of function mutation and consequential gain in the levels of HOXA5 and HOXA9 as key orchestrators of treatment failure. Again, CBM identified 3 novel therapies for this patient targeting patient-specific biomarkers (Table 3).
Conclusion: Even in biological subgroups of AML expected to have sensitive disease, induction failure is not rare. Fortunately, the CBM could identify causes of failure and suggest alternative therapies based on co-occurring genomic abnormalities to mitigate the ineffectiveness of standard induction regimens in patients with resistant disease despite their favorable biology. The identification of patient-specific resistance mechanisms characterizes a new therapeutic imperative founded on deep molecular diagnosis that promises to enhance disease outcomes, inform treatment planning, avoid adverse events from ineffective therapies, and reduce costs. Also, computational modeling identifies alternate therapy regimens for refractory patients by incorporating patient-specific disease biomarkers. For all the non-responders, CBM identified 3 potential therapies across each fusion subgroup. Although these combinations need further validation in the clinic, the Cellworks CBM biosimulation platform allows for precision medicine approaches that target patient-specific disease biomarkers and treatment resistance mechanisms.
Castro:Cellworks Group Inc: Consultancy. Nair:Cellworks Research India Private Limited: Current Employment. Grover:Cellworks Research India Private Limited: Current Employment. Kumar:Cellworks Research India Private Limited: Current Employment. Agarwal:Cellworks Research India Private Limited: Current Employment. Suseela:Cellworks Research India Private Limited: Current Employment. Gopi:Cellworks Research India Private Limited: Current Employment. Ganesh:Cellworks Research India Private Limited: Current Employment. Shyamasundar:Cellworks Research India Private Limited: Current Employment. Kulkarni:Cellworks Research India Private Limited: Current Employment. Sauban:Cellworks Research India Private Limited: Current Employment. Balla:Cellworks Research India Private Limited: Current Employment. Chafekar:Cellworks Research India Private Limited: Current Employment. Choudhury:Cellworks Research India Private Limited: Current Employment. Mundkur:Cellworks Group Inc.: Current Employment. Macpherson:Cellworks Group Inc.: Current Employment. Kapoor:Cellworks Research India Private Limited: Current Employment. Howard:Boston Scientific: Consultancy; Cellworks: Consultancy; EUSA Pharma: Consultancy; Sanofi: Consultancy, Other: Speaker; Servier: Consultancy, Other: Speaker.

