

Introduction: In patients with SARS-CoV-2 COVID-19 infection elevated D-dimers are associated with a poor prognosis. Although suggestive of DIC, the majority of patients do not fulfil ISTH criteria for DIC. Studies have demonstrated that when compared to D-dimer, fibrin monomers are more sensitive and specific when differentiating overt DIC from non-overt DIC. Our special coagulation laboratory (SCL) routinely measures soluble fibrin monomer complex (SFMC) as part of our DIC profile in samples with elevated D-dimers. Here we aimed to investigate the percentage of patients with COVID-19 infection with elevated SFMC as performed as part of the DIC profile.
Methods: Between April 1st 2020 and July 26, 2020 inpatients at the Mayo Clinic Rochester, MN campus with COVID-19 infection who underwent DIC testing in SCL were identified through SCL database. Patients were excluded if SARS-CoV2 PCR results were not available in the Mayo Clinic electronic medical record (EMR). DIC profile components include prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), fibrinogen and D-dimer. Reflex SFMC is performed if D-dimer is elevated. Data abstracted from EMR included results of laboratory tests, date of COVID-19 symptom onset, date of SARS-CoV2 PCR positivity, and death within 30 days of hospital admission. The ISTH DIC score was calculated and patients were labeled as overt DIC or non-overt DIC based off of ISTH DIC score ≥5.
Results: 35 patients (19 female), median age 59 years (28-91) met our study criteria DIC profiles were obtained 6.5 (1-37) days after COVID-19 symptom onset (n=33) with 28 obtained within 14 days of symptom onset. Time to DIC profile from SARS-CoV2 PCR testing was 4 (0-37) days (n=35) with 31 having testing completed within 14 days of PCR positivity. 8 patients were intubated during hospitalization and of the remaining 27, 67% required supplemental oxygen.
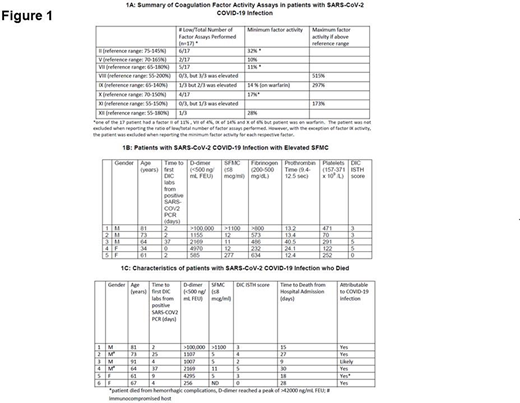
21/35 (60%) patients had an elevated fibrinogen (526.5 mg/dL (201-800)) while 19/35 (54%) had a prolonged PT (12.8 seconds (10.1-99.6) and 5/35 (14%) had a prolonged APTT (31 seconds (24-68)). 17 patients with prolonged PT and 3 patients with prolonged APTT had factor activity assays performed (Figure 1A). 9/35 (25%) had thrombocytopenia (230 x 109/L (12-709) and 27/35 (77%) patients had an elevated D-dimer (895 ng/ml FEU (220- >100,000). D-dimer was higher in males than in females (p: 0.049). Of those with elevated D-dimer only 5/27 (18.5%) had an elevated SFMC (5 mcg/ml (5- >1100) (Figure 1B).
4/35 (11%) patients had ISTH DIC scores ≥ 5 and all had score of 5. All of these patients had D-dimer > 2000 ng/ml while only 2 had elevated SFMC however SFMC in both of these patients was < 15 mcg/ml. Of these, one patient with SFMC of 12 mcg/ml had known cirrhosis and the other with an SFMC of 11 mcg/ml had acute decompensation and associated shock liver. This patient also had venous thrombosis 3 days prior to DIC profile and died from complications related to COVID-19 infection. Of the two other patients with high ISTH score and normal SFMC, one had previous chronic thrombocytopenia of < 50 x109/L while the other had concomitant admission for acute and recurrent pancreatitis in the setting of alcoholism with acute intoxication. Six patients died within 30 days of admission and in 2/5 performed SFMC was elevated (Figure1C).
Conclusion: Compared to 77% of patients with elevated D-dimers, of those tested only 18.5 % of patients had elevated SFMC. It has been hypothesized that the elevated D-dimer noted in COVID-19 pulmonary infection is a direct consequence of acute lung injury and not overt DIC. Although preliminary, the small percentage of patients with overt DIC by ISTH criteria and normal SFMC in the majority of the current cohort support this hypothesis; however studies in a larger more controlled cohort are needed to confirm these findings.
Sridharan:Alexion: Honoraria. Pruthi:Merck: Honoraria; Instrumentation Laboratory: Honoraria; HEMA Biologics: Honoraria; Bayer Healthcare: Honoraria; Genentech Inc.: Honoraria; CSL Behring: Honoraria.

