

Background: Tisagenlecleucel (tisa-cel), an autologous anti-CD19 chimeric antigen receptor (CAR)-T cell therapy, has demonstrated durable responses and a manageable safety profile in adult patients (pts) with relapsed/refractory diffuse large B-cell lymphoma (r/r DLBCL). It has previously been suggested that prior therapy with ibrutinib, a Bruton's tyrosine kinase (BTK) inhibitor, may improve tisa-cel manufacturing, in vivo cellular kinetics, and antitumor efficacy (Fraietta et al. Blood. 2016). Moreover, since BTK signaling is involved in direct pro-inflammatory polarization of macrophages, as well as indirectly by T cells, it is hypothesized that ibrutinib may mitigate CAR-T cell-related toxicities such as cytokine release syndrome (CRS) and neurological events (NE). We report the initial results from a Phase Ib, multicenter, open-label trial evaluating the safety and tolerability of tisa-cel in combination with ibrutinib in adult pts with r/r DLBCL.
Methods: Adult pts with r/r DLBCL who received >2 prior lines of systemic therapy, including pts who progressed after or were ineligible for autologous stem cell transplant, were enrolled. The study design has 2 nonrandomized arms. In Arm 1, pts received ibrutinib 560 mg/d for ~4 weeks prior to leukapheresis; in Arm 2, pts were exposed to ibrutinib after leukapheresis. In both arms, ibrutinib was continued throughout lymphodepleting chemotherapy, tisa-cel infusion, and post infusion for up to 24 months. Lymphodepleting chemotherapy, ending at least 2 days before tisa-cel infusion, was either fludarabine (25 mg/m2) and cyclophosphamide (250 mg/m2) daily for 3 days or bendamustine (90 mg/m2) daily for 2 days. Pts received a single infusion of tisa-cel (target dose: 0.6-6.0×108 viable CAR+ T cells). Primary endpoints are incidence and severity of adverse events and ibrutinib dose interruptions/modifications. Secondary endpoints include best overall response (BOR) by Lugano criteria and cellular kinetics of tisa-cel.
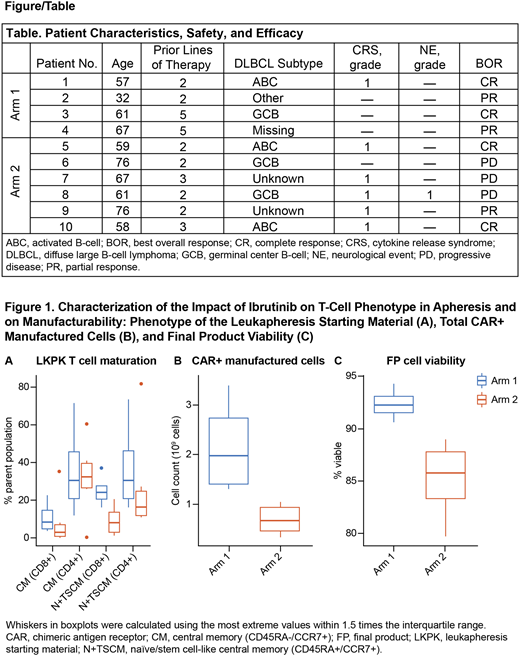
Results: As of June 9, 2020, 10 pts have been treated and observed through at least the Day 28 assessment: 4 in Arm 1 and 6 in Arm 2. Median age was 59 (range, 32-67) in Arm 1 and 64 (range, 58-76) in Arm 2. Median number of prior therapies was 3.5 (range, 2-5) in Arm 1 and 2 (range, 2-3) in Arm 2. Three of 10 pts (Arm 1, n=1; Arm 2, n=2) had an activated B-cell-like subtype of DLBCL. Six of 10 pts (Arm 1, n=1; Arm 2, n=5) had grade 1 CRS (by Lee scale) and 1 pt had NE (Arm 2, grade 1 by ASTCT criteria; Table). One pt in Arm 2 had grade 3 neutropenia lasting >28 days post tisa-cel infusion. No other pts had grade 3 or 4 neutropenia or thrombocytopenia lasting >28 days. No major bleeding events were observed. Ibrutinib-related bradycardia and atrial fibrillation (both grade 2) were each observed in 1 pt in Arm 1; supraventricular tachycardia (grade 1) related to tisa-cel was observed in 1 pt in Arm 2. No pt required tocilizumab or ICU admission. As of data cutoff, BOR in Arm 1 was complete response (CR) in 2 pts and partial response (PR) in 2 pts, with no relapses. BOR in Arm 2 was CR in 2 pts, PR in 1 pt, and progressive disease in 3 pts (Table). CAR-T cell expansion in vivo by qPCR was in line with data from the pivotal JULIET trial, except for 1 pt in Arm 2 whose transgene levels were below the limit of quantification at all points in time and who progressed at Day 28.
Median viability of the leukapheresis material was 96.80% (range, 88.8-97.3) in Arm 1 and 90.95% (range, 88.1-94.7) in Arm 2. A naïve/stem cell-like central memory phenotype (CD45RA+/CCR7+) was observed in 24.05% (median; range, 15.9-37.0) of CD8+ T cells in the leukapheresis material for Arm 1 and in 8.12% (median; range, 1.3-20.4) for Arm 2 (Fig.1A). Fig.1B shows total CAR+ manufactured cells in each arm. The median dose of the final product was 3.9×108 CAR+ T cells in Arm 1 (range, 3.4-4.6×108 CAR+ T cells; median viability 92.25%) and 1.7×108 CAR+ T cells in Arm 2 (range, 1.2-3.0×108 CAR+ T cells; median viability 85.8%; Fig.1C). IFNγ secretion of tisa-cel in vitro in response to CD19+ target cells was similar between the 2 arms, whereas median normalized IL-2 responses were 23.1 fg/CAR+ cell in Arm 1 (range, 16.7-43.8) and 1.1 fg/CAR+ cell in Arm 2 (range, 0-17.3).
Conclusions: These results support the feasibility of administering ibrutinib to pts with DLBCL throughout tisa-cel therapy. When given before apheresis, ibrutinib may improve CAR-T cell manufacturing, although further studies are needed to confirm this finding.
Chavez:AstraZeneca: Speakers Bureau; Morphosys: Consultancy, Speakers Bureau; Merck: Research Funding; Bayer: Consultancy; BeiGene: Speakers Bureau; Karyopharm: Consultancy; Genentech: Speakers Bureau; AbbVie: Consultancy; Epizyme: Speakers Bureau; Gilead: Consultancy; Celgene: Consultancy; Novartis: Consultancy; Kite, a Gilead Company: Consultancy, Speakers Bureau; Verastem: Consultancy; Pfizer: Consultancy. Locke:Kite, a Gilead Company: Consultancy, Research Funding; Calibr: Consultancy; Celgene/Bristol-Myers Squibb: Consultancy; Novartis: Consultancy; GammaDelta Therapeutics: Consultancy; Cellular Biomedicine Group: Other: Consultancy with grant options; Allogene: Consultancy; Wugen: Consultancy. Simon:Novartis: Current Employment. Lewandowski:Novartis Institutes for BioMedical Research: Current Employment. Awasthi:Novartis Institutes for BioMedical Research: Current Employment. Engels:Novartis Institutes for BioMedical Research: Current Employment. Georgala:Novartis Pharmaceuticals Corporation: Current Employment. Bondanza:Novartis Institutes for BioMedical Research: Current Employment. Schuster:AlloGene, AstraZeneca, BeiGene, Genentech, Inc./ F. Hoffmann-La Roche, Juno/Celgene, Loxo Oncology, Nordic Nanovector, Novartis, Tessa Therapeutics: Consultancy, Honoraria; Novartis, Genentech, Inc./ F. Hoffmann-La Roche: Research Funding.

