

Introduction: Mutations in the gene isocitrate dehydrogenase 2 (IDH2) occur in ~12-15% of patients with acute myeloid leukemia (AML). Enasidenib, an oral small molecule selective targeted inhibitor of IDH2 enzymes, was approved forIDH2mutated relapsed/refractory AML (RR-AML) in 2017 (Stein et. al., 2017). There is limited data regarding its efficacy and toxicity outside the context of clinical trials. Using Mayo Clinic's cohort of AML patients, we provide a real-world look at outcomes forIDH2mutated RR-AML patients treated with enasidenib.
Methods: A total of 13 patients treated with enasidenib for RR-AML were identified, all of which experienced at least one relapse following induction chemotherapy. Response assessment was based on European Leukemia Net (ELN) 2017 response criteria.Complete blood counts including blast percentage and transfusion dependency were obtained at AML diagnosis, initiation of enasidenib, 2 months and 6 months following initiation of therapy. Transfusion dependency was defined by the need for either a red cell or platelet transfusion within 4 weeks of the designated time frame. We compared the clinical characteristics of patients who achieved complete response (CR) (n=4) to those not achieving CR (n=9), using the Mann-Whitney U test for numerical variables and the Fischer's Exact test for quantitative data.
Results: The median age at diagnosis of our 13 patients was 68 years (range 60-82), with a male predilection (n=11) (Table 1). Cytogenetic and molecular genetic findings are provided in Table 2. Complete response (CR) was achieved in 4 (30.7%) patients by cycle 2 and 2 of those patients (50%) proceeded to an allogeneic hematopoietic stem cell transplant (AHSCT). The median time from diagnosis to initiation of treatment for patients in CR was 3.5 months (range 1-7), and for patients not achieving CR was 13 months (range 6-53; p=0.048), with median time of follow up after treatment initiation of 23.5 months (range, 5-36) and 7 months (range, 1-14), respectively. Among 8 patients who were transfusion dependent at baseline, all the CR patients (2/2) achieved red blood cell and platelet transfusion independence 6 months after treatment, instead only (3/6) 50% of those not in CR achieved transfusion independence (p=0.028).
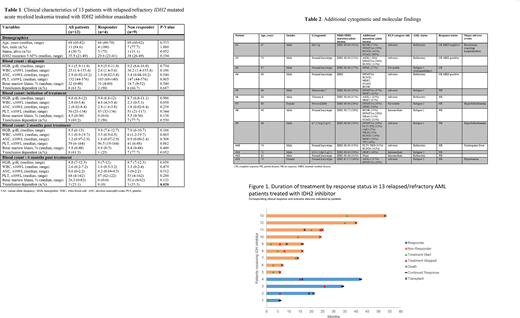
An initial trajectory of improvement in counts is noted from the time of diagnosis to the 2 month mark post treatment with 75% of the responder cohort showing improvement in counts which was durable through the 6 month mark, whereas 55% of those that did not respond had worsening counts at month 2 and died prior to 6 month follow up. At the time of data cut-off, the median duration of CR was 14 months (range, 2-33), with 3 of 4 (75%) of responders maintaining CR. Figure 1 details overall responses and outcomes in all 13 patients. None of the patients in our study experienced differentiation syndrome. Five patients were hospitalized in the course of treatment for infectious complications. Two patients were noted to have hyperbilirubinemia however there was no clear indication that this was secondary to enasidenib
Median overall survival for all 13 patients was 21 months (range, 6-53 months) with leukemia free survival of 7 months (range, 5-19 months). Furthermore, median overall survival for patients in CR was 27 months (range, 6-42), and those not in CR was 16 months (range, 6-53) (p=0.20). In addition, we observed that 75% of patients who attained CR are alive compared to 11.1% of those not in CR (p = 0.052).
Conclusion: We demonstrate a superior CR rate of 30.7% with enasidenib amongstIDH2mutated RR-AML patients compared with clinical trial data showing CR rate of 19.6% (Stein et. al., 2019) despite our patients being heavily pre-treated with median number of two prior therapies (range; 1-5) including prior AHSCT in 2 patients. Moreover, a subset of patients (2 of 4 in CR) were able to undergo ASCHT. Finally, the achievement of CR at 2 months after initiation of therapy serves as an appropriate time point for response assessment.
No relevant conflicts of interest to declare.

