

Abstract
Background: Survival after HSCT from HLA-identical siblings is inferior in SAA patients 30 years or older as compared with younger patients. In order to improve survival in patients >30 years, the use of a less toxic regimen including reduced doses of chemotherapy in combination with ATG, while adding fludarabine, might be an option to explore with the aim to reduce transplant-related mortality. In the unrelated donor setting, we previously showed that a regimen combining fludarabine, ATG, and low-dose cyclophosphamide (CY) provided encouraging disease-free survival in 38 patients (Bacigalupo et al, Bone Marrow Transplant 2005).
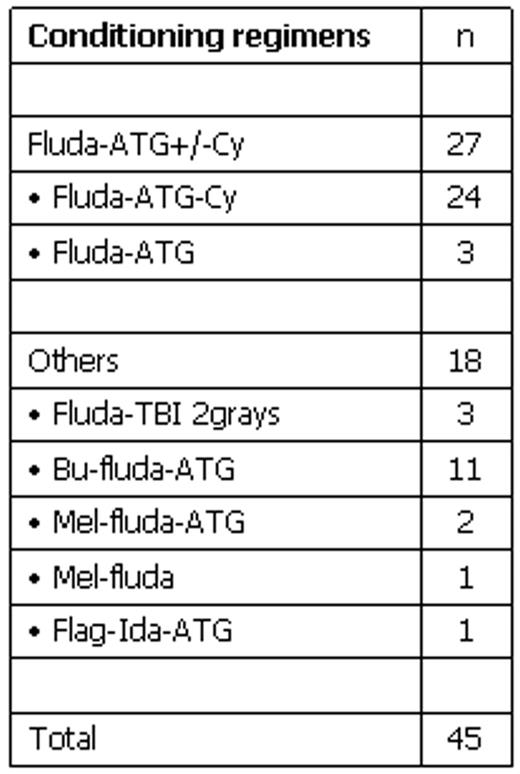
Patients and Method: In order to evaluate the toxicity profile, engraftment potential, and efficiency of HLA-identical HSCT using such fludarabine-based conditioning regimen, we conducted this study from the EBMT-SAA database, focussing on patients older than 30 years. From November 1996 to February 2005, 45 patients from 27 centres (median age 49 years, range 31–66 years) received HSCT for idiopathic SAA (n=40), or PNH clone-associated SAA (n=5). HSCT was performed either as first-line treatment (n=29), or after failure of ATG/ciclosporine (CsA) (n=10), or failure of a first allogeneic HSCT (n=6). The median interval between diagnosis and HSCT was of 10 months (range 1–350). Various fludarabine-based conditioning regimens were used (see Table), incorporating ATG +/− chemotherapy in the majority of patients (40 out of 45). We analyzed separately the outcome of patients receiving the combination of fludarabine, ATG and low-dose (<200 mg/kg) CY (n=27) from those receiving other fludarabine-based regimens (n=18). Marrow (n=21) or PBSC (n=24) grafts were unmanipulated. GVHD prophylaxis consisted of CsA/methotrexate (n=25), CsA alone (n=11), nothing (n=6), or other (n=3).
Results: All patients alive at d21 (n=41) engrafted with a neutrophil (ANC>500/μL) recovery occurring at a median of 16 days after transplant. Acute GVHD occurred in 16 patients with a maximum grade II in 11 patients and grade III-IV in 5. Among 33 evaluable patients, 11 developed chronic GVHD (extensive in 6). With a median follow-up of 21 months, the Kaplan-Meier overall probability of survival was of 54% ± 1%. Infections (n=5) and multi-organ failure (n=3) were the primary causes of death. In univariate (UV) and multivariate (MV) analyses incorporating patient- and transplant-related variables, the only factor significantly associated with better outcome was the type of conditioning, the fludarabine/ATG/low-dose CY combination providing a 77% ± 1% probability of survival versus 24% ± 1% with other regimens (p=.02 in UV and MV analyses).
Conclusion: Reduced intensity fludarabine-based conditioning regimen is feasible in SAA patients over the age of 30 and produces encouraging survival, especially when using a fludarabine, ATG and low-dose CY combination. A prospective trial is being conducted within the EBMT-SAAWP using this conditioning regimen.
Disclosure: No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal