

Abstract
Abstract 670
Richter syndrome (RS) represents the transformation of chronic lymphocytic leukemia (CLL) to aggressive lymphoma, most commonly diffuse large B-cell lymphoma (DLBCL). Knowledge of the genetic lesions associated with RS is scant and represents the aim of this study. The study was based on 47 RS cases (all DLBCL). In 32 cases, paired CLL/RS samples were available (28 clonally related and 4 clonally unrelated). In 15 cases, the sole RS sample was analysed. According to CD10/BCL6/MUM1 immunohistochemistry expression pattern, 43/47 (91.5%) RS were classified as non-germinal center DLBCL. At diagnosis, 37.8% RS showed ECOG PS >1, 77.8% Binet stage B-C, 95.7% Ann Arbor stage III-IV, 44.4% B symptoms, 45.7% tumor size >5 cm, 32.6% involvement of >1 extranodal site, 66.7% LDH elevation, and 28.9% platelets <100 × 10e(9)/l. RS treatment included CHOP-like regimens in 71.1% cases, rituximab-based immunochemotherapy in 44.4%, and allogeneic stem cell transplant in 8.9%. Candidate genetic lesions were selected among those recurrently affecting: i) de novo DLBCL; and ii) CLL. Mutational analysis of the TNFAIP3/A20, CARD11, BLIMP1, and TP53 genes was performed by direct DNA sequencing. Probes used for FISH analysis were: i) LSI13, LSID13S319, CEP12, LSIp53, LSIATM, LSI IGH/BCL2, LSI BCL6, LSI IGH/c-MYC/CEP8, LSI N-MYC (Abbott); BCL3 split signal (Dako): iii) 6q21/alpha-satellite (Kreatech Biotechnology); iv) BAC clones 373L24-rel and 440P05-BCL11A. Clonal relationship between CLL and RS samples was assessed by immunoglobulin gene rearrangement analysis. Among gene mutations that are associated with de novo DLBCL, TP53 mutations (exons 4-8) were identified in 18/46 (39.1%) RS, and CARD11 mutations (exons 5-9) in 3/44 (6.8%). Neither TNFAIP3/A20 (exons 2-9) nor BLIMP1 (exons 2-4) mutations were identified in RS. Among chromosomal abnormalities that are associated with de novo DLBCL, c-MYC translocation was observed in 2/17 (11.8%) RS, c-MYC amplification in 2/17 (11.8%), BCL6 amplification in 2/17 (11.8%), REL amplification in 1/10 (10.0%), and BCL2 amplification in 1/17 (5.9%). Neither BCL6 translocation, nor BCL2 translocation or BLIMP1 deletion were observed in RS. Among chromosomal abnormalities that are associated with CLL, 17p13 deletion (TP53) was observed in 5/17 (29.4%) RS, 11q22-q23 deletion (ATM) in 5/17 (29.4%), +12 in 4/17 (23.5%), 13q14 deletion (MIR15A/16B) in 2/17 (11.8%), BCL11A amplification in 1/10 (10.0%), BCL3 amplification in 2/17 (11.8%), BCL3 translocation in 1/17 (5.9%), and N-MYC amplification in 1/17 (5.9%). Analysis of paired clonally related CLL/RS samples showed that TP53 mutations and CARD11 mutations are acquired at RS transformation. Chromosomal abnormalities acquired at RS transformation included TP53 deletion (3/10, 30.0%), c-MYC translocation (2/10, 20.0%), BCL3 amplification (2/10, 20.0%), c-MYC amplification (1/10, 10.0%), BCL6 amplification (1/10, 10.0%), BCL2 amplification (1/10, 10.0%), and ATM deletion (1/10, 10.0%). To date, the sole tool for predicting RS survival is represented by the RS score, that is based on clinical variables (Tsimberidou et al, J Clin Oncol 2006; 24:2343). The notion that TP53 status predict survival in both CLL (Zenz et al, Blood 2008; 112: 3322; Rossi et al, Clin Cancer Res 2009; 15: 995) and de novo DLBCL (Young et al, Blood 2008; 112: 3088) prompted investigation of the impact of TP53 mutations on survival post RS transformation. Survival post transformation was significantly longer in RS devoid of TP53 mutations (27.0 months) compared to RS with TP53 mutations (9.4 months) (p=.023) (Fig. 1). Other variables associated with RS survival were age (p<.001), ECOG PS (p<.001), tumor size (p=.001), B symptoms (p=.001), platelet count (p=.002), Binet stage (p=.001), Rai stage (p=.001), and IPI (p=.008). Treatment strategy did not affect RS survival. Multivariate analysis selected TP53 mutations (HR:2.34; p=.028) as an independent predictor of RS survival along with variables identified by the RS score, including ECOG PS (p=.008), tumor size (p<.001), and platelet count (p=.004) . The conclusions of our study are multifold: i) the genetic profile of RS differs from that of de novo DLBCL; ii) few lesions are shared by RS and de novo DLBCL, including CARD11 mutations, c-MYC translocation and REL amplification; iii) TP53 mutations are the most frequent genetic lesion in RS; iv) TP53 mutations are an independent prognostic factor in RS. 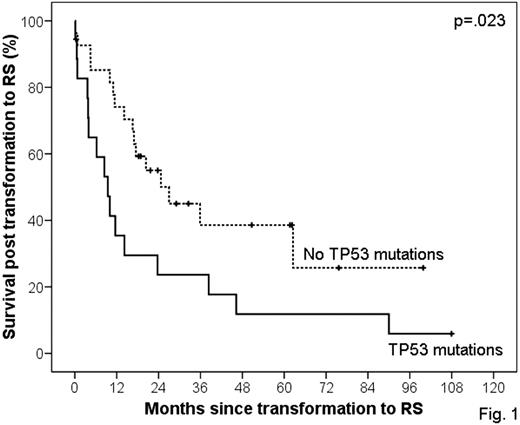

Disclosures:
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal