

Abstract
Sickle cell anemia (HbSS) is characterized by chronic hemolysis, i.e. a shortened red blood cell (RBC) lifespan. Hemolysis varies greatly in degree among patients and is thought to be the proximate cause of some of the complications of HbSS. To date, clinical studies exploring the pathological role of hemolysis in SCD have used surrogates (e.g., reticulocyte count, LDH, AST) rather than direct measures. Surrogate markers are inadequate to study causation, but current gold standard methods for calculating RBC lifespan in humans are labor-intensive and involve radioactivity or ex vivo cell labeling. Glycine is a precursor for both the globin and heme components of hemoglobin (Hb), so stable isotope-labeled glycine (15N-glycine) can be used to measure RBC survival. Following ingestion of 15N-glycine, labeled Hb is synthesized within RBC precursors that are subsequently released as an age cohort into the circulation where the label can be measured over time. This differs from population labels, e.g. chromium or biotin, that label RBCs of all ages in the circulation. The measurement is safe (no infusion of manipulated RBC products or radioactivity), not labor-intensive (no ex vivo manipulation of RBCs) and appears to be practical for use in clinical studies.
To measure RBC survival using 15N-glycine in patients with HbSS and demonstrate its practicality for use in multi-institutional clinical studies.
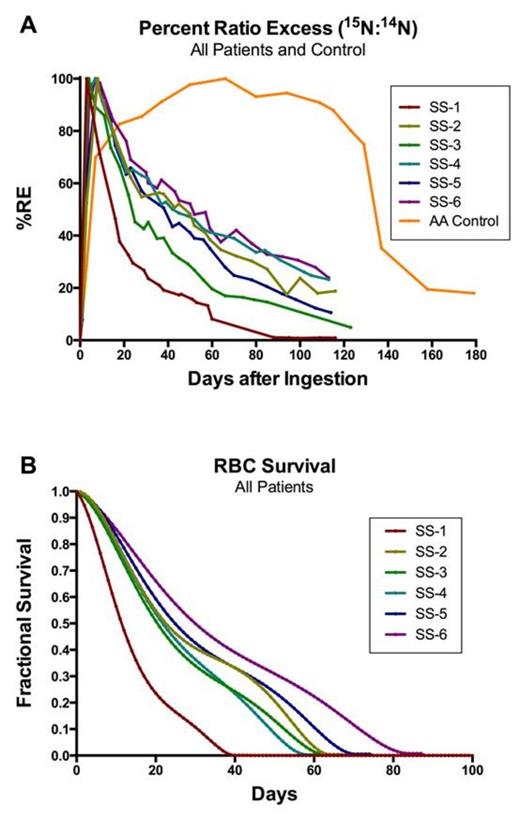
We enrolled individuals with HbSS in steady-state without hepatobiliary disease who had not been transfused in the preceding 3 months. After obtaining informed consent and duplicate baseline blood samples, participants ingested 15N-glycine and had serial phlebotomies over 16 weeks for blood counts, clinical chemistries, and storage of aliquots of frozen whole blood. Heme was extracted from frozen whole blood and analyzed using combustion isotope ratio mass spectroscopy at a commercial laboratory to give a precise ratio of 15N/14N, which is directly related to the number of cells remaining from the age cohort of RBCs that were produced in the presence of 15N-glycine. We defined the starting point for all RBC survival calculations as the time at which the percent ratio excess of 15N to 14N (%RE) reached 50% of the maximum value, and we defined the endpoint as the time at which the rate of change of %RE had decreased to 0.5% per day. To produce normalized RBC survival curves, the absolute %RE was corrected for any residual component evident at the endpoint by assuming a linear increase in the residual from the starting point to the endpoint. The normalized RBC survival curve was fit using a 5-order polynomial expression. Median survival, mean survival and mean RBC age were computed (Lindsell 2008).
Six participants with HbSS were studied. Mean age was 22.3 years (range 16-31); 4 of 6 were female; and 5 of 6 were prescribed a stable dose of hydroxyurea. All participants completed the 16-week protocol. None had a transfusion during the study, but one was hospitalized for a painful event. Curves for %RE (Figure, panel A) and normalized RBC survival (Figure, panel B) were generated. A representative individual with normal (AA) Hb type is shown (Figure, panel A) illustrating the more rapid rise and decline in %RE in HbSS, as expected physiologically. Median RBC survival was 21.6 days (S.D. 5.5; range 12.0- 28.3). Mean RBC survival was 26.6 days (S.D. 4.2; range 14.1- 36.0). Mean RBC age was 19.9 days (S.D. 5.1; range 11.4- 26.6). Reticulocyte count was significantly correlated with median RBC survival (Spearman rho = -0.943, P=0.005), mean RBC survival (rho = -0.943, P=0.005), and mean RBC age (rho = -0.886, P=0.019). Hb concentration, percent Hb F, LDH, AST, and total bilirubin were not significantly correlated with RBC survival in this small sample of 6 persons. Samples after 80 days added no useful information, so the number of phlebotomies can be decreased for future analyses.
This 15N-glycine stable isotope cohort label can measure RBC survival and quantify hemolysis safely and easily in patients with HbSS. This method is practical for use in multi-institutional clinical studies because whole blood can be frozen and stored for later shipment to central labs for processing and analysis. The causal role of hemolysis in the development of complications of HbSS can be studied without sole reliance on surrogate markers.
Lindsell CJ et al. Am J Hematol. 83(6):454-7, 2008.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal