

Abstract
Therapeutic options for limited-stage diffuse large B cell lymphoma (DLBCL) include short-course R-CHOP +/- IFRT and full-course R-CHOP +/- IFRT. In the rituximab-era, few randomized prospective studies exist to compare these treatment approaches in limited-stage DLBCL. In this retrospective analysis of limited-stage DLBCL, we report 1) prognostic factors associated with outcome and treatment and 2) outcomes associated with different treatment programs including 3-4 cycles of R-CHOP +/- IFRT and 6 cycles of R-CHOP +/- IFRT.
Patients with newly diagnosed limited-stage DLBCL treated at Memorial Sloan-Kettering Cancer Center with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) chemotherapy with or without involved-field radiotherapy from 1999 – 2012 were included. Limited-stage DLBCL was defined as Ann Arbor stage I or stage II, non-bulky (any mass < 10 cm). Patients with primary mediastinal large B-cell lymphoma were excluded. Treatment programs included: A) R-CHOP x3-4 cycles, B) R-CHOP x3-4 cycles + IFRT, C) R-CHOP x6 cycles, and D) R-CHOP x6 cycles +IFRT.
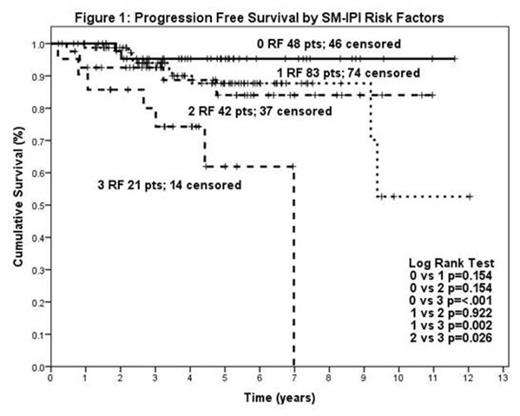
262 pts were identified with median age 58 years (range 18-85), 55% female (N=145), and 30% stage I (N=82), 37% Stage IE (N=96), <1% stage IXEE (N=1), 18% stage II (N=46), and 14% Stage IIE (N=37). The factors associated with inferior progression-free survival (PFS) were age > 60 (p=0.039), elevated LDH (p=0.014), and stage II disease (p=0.015). In contrast, female sex (p=0.54), B-symptoms (0.74), presence of extranodal “E” lesion (p=0.12), and poor performance status (0.35) were not significantly associated with PFS. The stage-modified IPI (SM-IPI, including the factors: stage II (vs. I), age>60, elevated LDH, and ECOG performance status ≥2) stratified patients into prognostically relevant groups, see Figure 1. In the rituximab era, the poorest outcomes were observed in patients with SM-IPI=3 (n=21). Interim PET imaging after 3-4 cycles (interpreted with International Harmonization Project criteria) was available in 198 patients. The majority of patients achieved a negative interim PET scan, see Table 1. Positive interim PET imaging was not associated with inferior PFS, p=0.45.
Among the 4 treatment programs, 17 patients received R-CHOP x3-4 cycles (A), 147 received R-CHOP x3-4 cycles + IFRT (B), 48 received R-CHOP x6 cycles (C), and 50 received R-CHOP x6 cycles +IFRT (D). Physician treatment choice appeared to be associated with clinical characteristics at presentation. To assess the clinical and demographic features associated with receipt of arm B versus C (analogous to the treatment arms in the historical study of chemotherapy versus combined modality therapy in the pre-rituximab era, SWOG 8736 (Miller, NEJM, 1998)), Chi-Square or Fisher exact tests were performed. Patients with stage II vs. I (p<0.001), B-symptoms (p<0.001), elevated LDH (p=0.03), and poor performance status (p=0.013) were significantly more likely to receive R-CHOP x6cycles versus R-CHOP x3-4cycles + IFRT. Therefore, patients with more advanced stage, systemic symptoms related to lymphoma, and elevated LDH were significantly more likely to receive full-course chemotherapy.
At median follow up of 4.7 years, the outcomes were excellent with 89% PFS and 94% OS for the entire cohort. There were 30 patients who progressed or died. Of the total 19 deaths, 7 were attributable to progressive lymphoma. The outcomes were similar for the 4 treatment groups, see Table 1. Among elderly patients, either ≥ 70 years (n=65) or ≥ 60 years (n=125), there were no differences in outcomes between treatment arms.
| Survival (%) at Median Follow-Up (4.7 yrs) | Interim PET (N=198) | |||
|---|---|---|---|---|
| Treatment | PFS | OS | DFS | Negative |
| R-CHOP x3-4 (N= 17) | 88.0 | 94.1 | 88.2 | 71% (5/7) |
| R-CHOP x3-4 + IFRT (N= 147) | 89.8 | 94.2 | 94.5 | 80% (106/131) |
| R-CHOP x6 (N= 48) | 85.6 | 89.4 | 92.9 | 78% (25/ 32) |
| R-CHOP x6 + IFRT (N= 50) | 90.1 | 97.9 | 90.1 | 64% (18/28) |
| Survival (%) at Median Follow-Up (4.7 yrs) | Interim PET (N=198) | |||
|---|---|---|---|---|
| Treatment | PFS | OS | DFS | Negative |
| R-CHOP x3-4 (N= 17) | 88.0 | 94.1 | 88.2 | 71% (5/7) |
| R-CHOP x3-4 + IFRT (N= 147) | 89.8 | 94.2 | 94.5 | 80% (106/131) |
| R-CHOP x6 (N= 48) | 85.6 | 89.4 | 92.9 | 78% (25/ 32) |
| R-CHOP x6 + IFRT (N= 50) | 90.1 | 97.9 | 90.1 | 64% (18/28) |
In the rituximab-era, short-course immunochemotherapy followed by radiation appears to have equivalent efficacy when compared to long-course immunochemotherapy in this selected population of limited-stage DLBCL patients. Prospective randomized studies are needed to define the optimal treatment for limited-stage DLBCL in the rituximab era.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal