

In this issue of Blood, report a pilot study in chronic lymphocytic leukemia (CLL) of stepping down the dose of ibrutinib over the initial 3 cycles of treatment and demonstrate that its relevant cellular biologic effects are maintained at lower doses.1 This study builds on the earlier observation that levels of Bruton’s tyrosine kinase (BTK), the target of ibrutinib, decrease during treatment.2 The therapeutic effect of ibrutinib is due to ligation of B-cell receptor (BCR) signaling by binding and irreversibly inhibiting BTK in the BCR signaling cascade.3 Therefore, if levels of BTK are decreased, the amount of ibrutinib necessary to achieve the same target occupancy should be less. To test this hypothesis, Chen et al designed a pilot study of ibrutinib dose reduction from 420 mg to 280 mg and then 140 mg over the first three 28-day cycles of treatment and examined the pharmacokinetics and pharmacodynamics at all dose levels.
Ibrutinib dose was sequentially decreased from the standard dose in CLL of 420 mg down to 140 mg by cycle 3. Mean plasma and intracellular ibrutinib levels as well as target occupancy were determined showing that target occupancy was maintained at >97% at all levels. ns, not significant. The figure has been adapted from Figures 1 and 2 in the article by Chen et al that begins on page 2249. Professional illustration by Patrick Lane, ScEYEnce Studios.
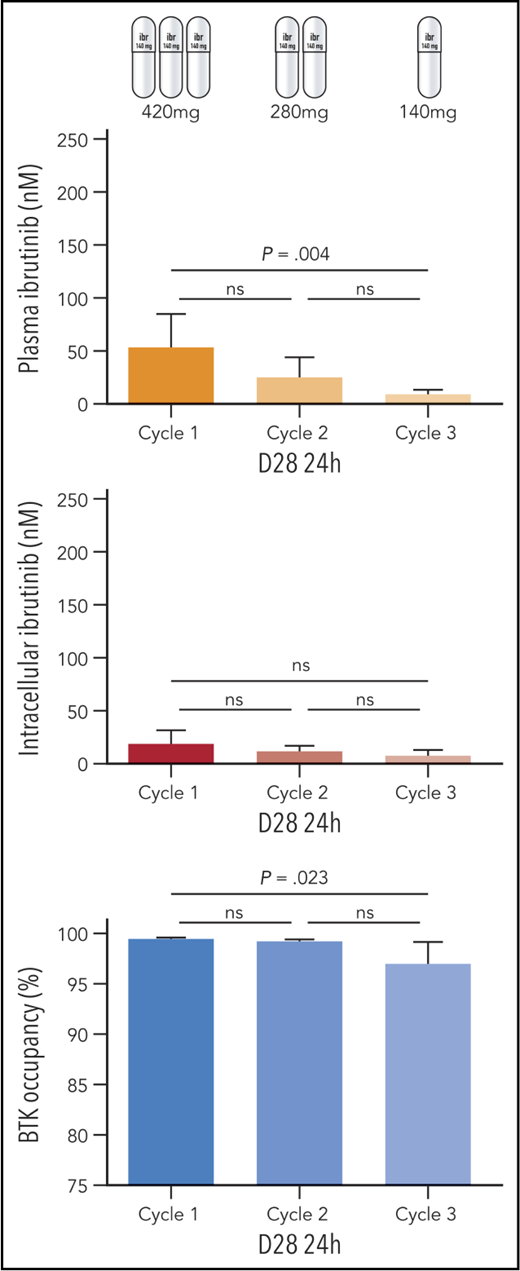
Ibrutinib dose was sequentially decreased from the standard dose in CLL of 420 mg down to 140 mg by cycle 3. Mean plasma and intracellular ibrutinib levels as well as target occupancy were determined showing that target occupancy was maintained at >97% at all levels. ns, not significant. The figure has been adapted from Figures 1 and 2 in the article by Chen et al that begins on page 2249. Professional illustration by Patrick Lane, ScEYEnce Studios.
Low-dose ibrutinib is an enticing concept as reduced doses are likely to have reduced toxicity, both physical and financial. The cost and the side effects of ibrutinib are common reasons for treatment discontinuation and prevent CLL patients from realizing the maximal benefit from this disease-altering therapy.4 This makes investigation of decreased doses highly attractive. The idea that lower-dose ibrutinib may be as effective as the standard dose of 420 mg daily is supported by a retrospective study of patients who had a dose reduction for clinical reasons and had a similar progression-free survival compared with those who remained at full dose.5
This study by Chen et al is small, enrolling 11 patients, and includes strictly laboratory data. Patients with CLL who required treatment were enrolled, and ibrutinib was started at 420 mg, which is the licensed dose in CLL. The dose of ibrutinib was then systematically reduced at the beginning of each cycle, and samples were collected at multiple time points for measurement of plasma and intracellular drug levels as well as BTK occupancy (see figure). Although plasma and intracellular ibrutinib levels were lower at lower doses as expected, mean BTK occupancy remained >97% even at the farthest time point, which was cycle 3 day 28 at 24 hours after dosing.
The analysis was not limited to target occupancy, and the major strength of this work is the diversity and completeness of pharmacodynamic end points examined. Comparison with baseline values was used to determine effect over each cycle. In addition to confirming that BTK protein levels decreased as expected, blockade of BCR signaling was demonstrated at all doses using standard immunoblotting techniques to detect phosphorylation of BTK and PLCγ2, the immediate downstream target of BTK. Further evidence for loss of BCR signaling activity was also shown by decreases in plasma CCL3 and CCL4 chemokine levels. Changes in Bcl-2 family proteins and NF-κB signaling characteristic of BCR inhibition and previously demonstrated during ibrutinib treatment were also observed. These changes in biologically relevant markers certainly provides ample evidence that ibrutinib is active at these lower doses after employing this step-down strategy.
However, enthusiasm for ibrutinib dose reduction must be tempered by the fact that there were no clinical end points in this study, and duration of follow-up was short at <3 months. It is important to realize what these data do not demonstrate. The study was not designed to examine for potential differences in response, adverse events, or development of resistance at the lower doses of ibrutinib compared with the standard 420-mg dose. Data from this small study with only laboratory end points are insufficient to recommend ibrutinib dose reduction in routine clinical practice except when required to manage intolerable side effects. Given the financial burden of ibrutinib, which is a frequent concern of patients, it will be tempting to consider a lower-dose approach, and this must be resisted until a study with clinical end points is completed.
This pilot data support that a larger clinical trial with ibrutinib step-down dosing is warranted, and it is imperative that this study be done. Ideally this would be a randomized trial comparing reduction to 140 mg to the standard 420 mg so that differences in response profile, progression-free survival, and toxicity can be determined. If a prospective study were to demonstrate equivalent clinical outcomes with lower doses of ibrutinib, this would be a major benefit to patients by sparing side effects and cost, as well as lessen the burden on the health care system, where the economic impact would be substantial. This study by Chen et al is an important step toward this possibility.
Conflict-of-interest disclosure: K.A.R. receives research funds from Genentech and consulted for Acerta.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal