

Abstract
Introduction: A new 3-group clinical classification schema proposed by the International Consortium (Blood 2016,128:4320) and subsequently validated by the MDS Düsseldorf Registry (Leukemia Research 2017,55:S149) was shown to independently stratify Chronic Myelomonocytic Leukemia (CMML) patients with regard to prognosis. The groups were defined as follows: 1. Myelodysplastic (MD)-CMML: WBC ≤10 x 109/L, circulating immature myeloid cells (IMC) = 0, no splenomegaly; 2. MD/MP (overlap) -CMML: WBC 10-20 x 109/L or WBC ≤10 x 109/L but IMC>0 and/or splenomegaly; 3. Myeloproliferative (MP)-CMML: WBC >20 x 109/L. The aim of this study was to determine the impact of this new classification schema on the outcome of allogeneic hematopoietic stem cell transplantation (HSCT), still representing the only curative option for eligible patients with CMML. Since time from diagnosis to transplant is highly variable with clinical data being highly dependent both on the disease natural history and on pretransplant treatments, in this study the group classification was based on the data registered at time of transplantation.
Patients and Methods: Patients who had received a first allogeneic HSCT for CMML between 1997 and 2016 were selected from the EBMT database. Following the exclusion of patients transformed into AML at the time of transplant, 1614 patients were initially included. However, since information on spleen assessment was reported only in 9.4% of patients (with splenomegaly in 22.5% of them), the final number of patients included in the analysis, with IMC replaced by peripheral blasts (PB), was 151. Survival of this group of patients and the remaining 1463 for whom spleen, WBC and PB data were not reported were almost identical, therefore validating the assumption that the study population included in the analysis was representative of the whole study population with respect to survival. Impact of the new classification on HSCT outcome was analyzed regarding OS and PFS, cumulative incidence of relapse and NRM (gray test).
Results: 98 male (64.9%) and 53 female (35.1%) patients were included to the study. Median age at HSCT was 60 years (range 20-75). At time of HSCT, 39 (26.2%) patients were in complete remission, whereas 110 (73.8%) had active disease (2 missing). Matched related donor HSCT was performed in 29.1% of the patients, matched unrelated donor HSCT in 60.9%, mismatched related in 4% and mismatched unrelated in 6%. Bone marrow (8%), peripheral blood (90%), or cord blood (2%) served as the stem cell source. Myeloablative preparative regimens were used in 30.5% of patients, whereas reduced intensity regimens were given to 69.5% of patients. Median survival of patients included into this study was 17 months (95% CI 13-38). According to the new classification schema, 57 (37.7%) patients were classified as MD-CMML, 64 (42.4%) as MD/MP-CMML and 30 (19.9%) as MP-CMML. With regard to the above-mentioned patients' characteristics, no significant differences were detected among groups with the only exception of disease status at HSCT: indeed, patients in CR were 41.1%, 23.4% and 3.4% respectively in MD-, MD/MP-, and MP-CMML (p=0.001). According to the WHO categories, 51% of patients were classified as CMML-0, 29% as CMML-1 and 20% as CMML-2%.
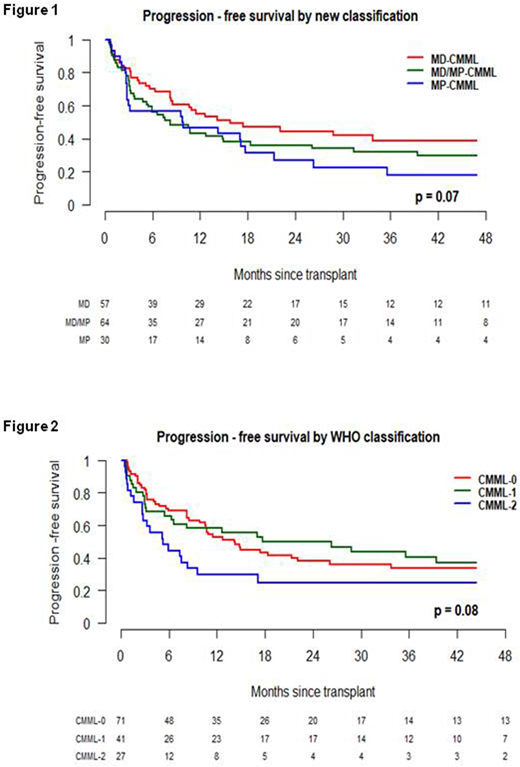
By univariate analysis, the new clinically-based classification was found to associate with PFS with borderline statistical significance (Log-Rank test 0.07) [Figure 1], while no difference was detected in terms of OS, cumulative incidence of relapse and cumulative incidence of NRM, possibly due to the relatively small number of patients. Of note, by lumping together the MD/MP and MP categories, the difference in the PFS with the MD-CMML group achieves statistical significance (p=0.036). In contrast, the WHO classification was able to clearly separate CMML-2 as having a significant worse OS in comparison to the CMML-0/CMML1 patients (whose curves were superimposable), whereas no significant differences were detected for PFS [Figure 2], relapse incidence and NRM.
Conclusions: Although performed on a limited number of patients, in this retrospective analysis we show that CMML patients categorized as MD-CMML according to the new clinically-based classification underwent allo-HSCT with a significantly higher proportion of CR and had a significantly better PFS in comparison to patients with overlap or proliferative characteristics.
Finke:Neovii: Consultancy, Honoraria, Other: travel grants, Research Funding; Novartis: Consultancy, Honoraria, Other: travel grants, Research Funding; Riemser: Consultancy, Honoraria, Research Funding; Medac: Consultancy, Honoraria, Other: travel grants, Research Funding. Beguin:Kiadis Pharma: Consultancy. Ganser:Novartis: Membership on an entity's Board of Directors or advisory committees. Russell:Daiichi Sankyo: Consultancy; Jazz Pharma: Speakers Bureau; Pfizer: Consultancy, Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal