


Abstract
Intensive therapies are often medically indicated for older adults with hematologic malignancies. These may include induction chemotherapy for acute myeloid leukemia (AML), as well as autologous hematopoietic cell transplant (autoHCT) and allogeneic hematopoietic cell transplant (alloHCT). However, it is not always clear how to best deliver these therapies, in terms of determining treatment eligibility, as well as adjusting or adding supportive measures to the treatment plan to maximize successful outcomes. Beyond performance status and presence of comorbidities, comprehensive geriatric assessment and individual geriatric metrics have increasingly been used to prognosticate in these settings and may offer the best approach to personalizing therapy. In the setting of AML induction, evidence supports the use of measures of physical function as independent predictors of survival. For patients undergoing alloHCT, functional status, as measured by instrumental activities of daily living (IADL) and gait speed, may be an important pretransplant assessment. IADL has also been associated with post-autoHCT morbidity and mortality. Current best practice includes assessment of relevant geriatric metrics prior to intensive therapy, and work is ongoing to develop complementary interventions.
Introduction
The approach to determining treatment tolerance for older adults with hematologic malignancy often differs significantly from that for solid tumor patients. Treatment of hematologic malignancies involves relatively more intensive chemotherapy, commonly given in the hospital setting and with longer duration of myelosuppression. The definition of “older” is generally younger in the hematologic malignancies; in acute myeloid leukemia (AML), for example, “older” is often defined as >60 years, whereas in lung or colon cancer, studies of older patients usually focus on those >70 years or even >80 years. The average age at diagnosis of these malignancies is not meaningfully different,1 but the toxicities associated with some of our therapies for hematologic malignancies are such that we are forced to think carefully about treatment tolerance in a relatively younger patient subset.
In addition to therapies for hematologic malignancies being relatively more intensive, they are somewhat less easily amenable to meaningful modification because of their very nature. For example, an allogeneic hematopoietic cell transplant (alloHCT) still carries quite a formidable set of risks, even in the nonmyeloablative setting. An autologous transplant is inherently myeloablative, even if the chemotherapy dose is modified for age or organ function. How then do we best deliver intensive therapies to older adults with hematologic malignancies? How do we determine candidacy for an intensive therapy and then how can we adjust our treatment or supportive care to ensure patient tolerance? In this review, I will discuss the existing data addressing these questions and best practices in the setting of AML induction chemotherapy, allogeneic transplant, and autologous transplant and will briefly discuss what is known about older patients receiving chimeric antigen receptor (CAR) T-cell therapy.
Clinical case 1: part 1
Patient 1 is a 68-year-old woman who presented with shortness of breath for 1 week. Complete blood count showed pancytopenia, and the differential was notable for 30% circulating blasts. Bone marrow biopsy revealed 70% myeloid blasts consistent with AML. Cytogenetics were positive for trisomy 8 and trisomy 11, and molecular testing was negative for FLT3, NPM1, CEBPA, IDH1/2, and TP53 mutations.
The patient’s medical history was notable for hypertension, hyperlipidemia, diabetes mellitus, celiac disease, and gastroesophageal reflux disease. Her surgical history included hysterectomy and cholecystectomy. At the time of presentation of her AML she was taking 10 medications, including 3 antihypertensives, aspirin, a statin, and metformin. She had been working as a school teacher up until the time of her diagnosis.
How to evaluate an older AML patient for induction
The decision that is required for the above patient at presentation is whether she is “fit” for intensive induction chemotherapy, such as 7+3 (7 days of cytarabine 100-200 mg/m2 and 3 days of an anthracycline). Historically, efforts have been made to address this question by using algorithms to determine the probability of complete remission, early mortality, and survival.2-5 The algorithms differ somewhat but generally incorporate chronologic age, performance status, and cytogenetic/molecular data. Although useful, these algorithms have their limitations. One is the reliance of most on cytogenetic/molecular data, which often are not available at the time a treatment decision is being made. A second limitation is the use of chronologic age. Although clearly a strong predictor of outcomes, chronologic age is a surrogate for other quantifiable characteristics, including clinical variables, comorbidities, functional limitations, and frailty. Indeed, in 1 study, the inclusion or exclusion of age from a multivariate model did not significantly affect predictive ability when other clinical variables were included. Likely in part for these reasons, algorithms predicting remission or induction mortality have not been widely adopted in clinical practice as decision-making tools.
A truly individualized or personalized decision regarding induction chemotherapy in an older patient must take into account comorbidities, as well as physical and functional limitations, at a minimum. These are known as geriatric domains, and they can be measured individually or as part of a comprehensive geriatric assessment (CGA). CGA is a standardized battery of assessments designed to measure geriatric domains, including functional status, comorbid conditions, cognition, psychological or mental health, social support, nutritional status, and polypharmacy. CGA has been shown to be feasible in the setting of AML induction chemotherapy, in the single-institution and in the multicenter cooperative group setting, taking 30 to 45 minutes to complete.6,7 However, if CGA is not available, even single-domain measures may provide additional prognostic value. Table 1 summarizes the evidence supporting the prognostic value of geriatric domains in older patients with AML undergoing intensive induction, and select geriatric measures of physical function8-10 are displayed in Figure 1.
Evidence supporting the prognostic value of geriatric domains and specific metrics in older AML patients
| Metric | References | Outcome | Patients | Therapy | Data source |
|---|---|---|---|---|---|
| Comorbidities | |||||
| CCI | 11 | ED, CR, OS | n = 133, age ≥ 70 y | Intensive | Retrospective |
| 12 | ED, OS | n = 5480, age ≥ 65 y | Variable | Registry | |
| 13 | No effect on ED, CR | n = 2792, all ages | Variable | Registry | |
| 14 | No effect on ED, OS | n = 144, age ≥ 60 y | Intensive | Retrospective | |
| HCTCI | 15 | ED, OS | n = 177, age ≥ 60 y | Intensive | Retrospective |
| 16 | OS | n = 416, age ≥ 65 y | Intensive | Retrospective | |
| 17 | ED, OS | n = 80, age > 55 y | Intensive | Retrospective | |
| Augmented HCTCI | 18 | ED, OS | n = 1100, all ages | Variable | Retrospective |
| Diabetes | 14 | ED | n = 144, age ≥ 60 y | Intensive | Retrospective |
| Physical function | |||||
| IADL | 19 | OS | n = 63, all ages | Variable | Prospective |
| 20 | OS | n = 101, age ≥ 65 y | Variable | Retrospective | |
| ADL | 21 | OS | n = 195, age ≥ 60 y, AML and MDS | Variable | Prospective |
| SPPB | 22 | OS | n = 74, age ≥ 60 y | Intensive | Prospective |
| Modified SPPB | 23 | No effect on OS | n = 97, age ≥ 60 y | Intensive | Prospective |
| Cognition | |||||
| Modified MMSE | 22 | OS | n = 74, age ≥ 60 y | Intensive | Prospective |
| Polypharmacy | |||||
| No. medications | 24 | ED, CR, OS | n = 150, age ≥ 60 y | Intensive | Retrospective |
| Metric | References | Outcome | Patients | Therapy | Data source |
|---|---|---|---|---|---|
| Comorbidities | |||||
| CCI | 11 | ED, CR, OS | n = 133, age ≥ 70 y | Intensive | Retrospective |
| 12 | ED, OS | n = 5480, age ≥ 65 y | Variable | Registry | |
| 13 | No effect on ED, CR | n = 2792, all ages | Variable | Registry | |
| 14 | No effect on ED, OS | n = 144, age ≥ 60 y | Intensive | Retrospective | |
| HCTCI | 15 | ED, OS | n = 177, age ≥ 60 y | Intensive | Retrospective |
| 16 | OS | n = 416, age ≥ 65 y | Intensive | Retrospective | |
| 17 | ED, OS | n = 80, age > 55 y | Intensive | Retrospective | |
| Augmented HCTCI | 18 | ED, OS | n = 1100, all ages | Variable | Retrospective |
| Diabetes | 14 | ED | n = 144, age ≥ 60 y | Intensive | Retrospective |
| Physical function | |||||
| IADL | 19 | OS | n = 63, all ages | Variable | Prospective |
| 20 | OS | n = 101, age ≥ 65 y | Variable | Retrospective | |
| ADL | 21 | OS | n = 195, age ≥ 60 y, AML and MDS | Variable | Prospective |
| SPPB | 22 | OS | n = 74, age ≥ 60 y | Intensive | Prospective |
| Modified SPPB | 23 | No effect on OS | n = 97, age ≥ 60 y | Intensive | Prospective |
| Cognition | |||||
| Modified MMSE | 22 | OS | n = 74, age ≥ 60 y | Intensive | Prospective |
| Polypharmacy | |||||
| No. medications | 24 | ED, CR, OS | n = 150, age ≥ 60 y | Intensive | Retrospective |
ADL, activities of daily living; CCI, Charlson Comorbidity Index; CR, complete remission; ED, early death; HCTCI, Hematopoietic Cell Transplant Comorbidity Index; IADL, instrumental activities of daily living; MMSE, Mini-Mental Status Examination; OS, overall survival; SPPB, Short Physical Performance Battery.
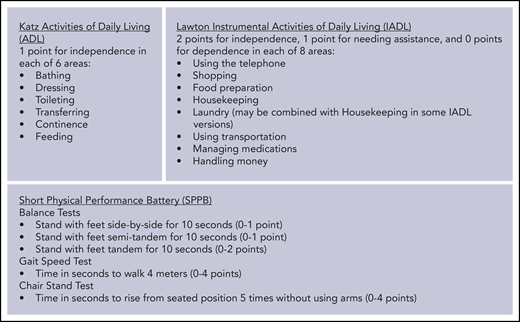
Select geriatric metrics assessing physical function. Adapted from Katz et al,8 Lawton et al,9 and Guralnik et al.10
Comorbidities are clearly an important component of treatment decision making, although data supporting the use of comorbidity indexes are not consistent. This is likely due to the low proportion of patients with high comorbidity scores who received intensive therapy (5%-25%),13,16 suggesting that comorbidities did influence physicians’ treatment decisions but making it difficult to study retrospectively. One study has demonstrated that diabetes, in particular, may increase the risk of early death in older adults receiving intensive induction.14
The geriatric domain with the best evidence supporting additional prognostic value beyond performance status and comorbidities is physical function. This can be measured subjectively by patient report of activities of daily living (ADL; examples include bathing and dressing) or instrumental activities of daily living (IADL; examples include grocery shopping and managing money). Alternatively, physical function can be measured objectively using specific testing, such as the Short Physical Performance Battery (SPPB; includes measures of balance, walk speed, and chair rises). Studies looking at ADL or IADL in AML patients have shown an independent association with survival, but they are limited by inclusion of patients receiving high- and low-intensity treatments; in 1 study myelodysplastic syndrome patients were also included.19-21 One study of patients receiving intensive induction showed that SPPB score < 9 (range, 0-12) was an independent predictor of survival22 ; however, a second study looking at a modified version of the SPPB did not show such an association.23 This difference could be explained by differences in the patient populations or the details of the SPPB modification. Cognition and polypharmacy, 2 other geriatric domains, have each been shown in single studies to predict survival independently in intensively treated AML patients, with polypharmacy (defined as number of medications ≥ 4) also predicting early death and achievement of remission.22,24
Considering the alternatives to induction
The decision to pursue induction chemotherapy must not only consider its merits and risks, but also the merits and risks of alternatives to induction. The same geriatric vulnerabilities that may influence tolerance of intensive therapy may also influence tolerance of nonintensive therapy. Little data exist prospectively comparing induction chemotherapy, such as 7+3, directly with lower-intensity treatment options, such as a hypomethylating agent (HMA), although the ongoing EORTC AML21 trial is randomizing patients between intensive induction and 10 days of decitabine and includes assessment of the prognostic value of ADL and SPPB (NCT02172872). Recently, multiple new drugs have been approved for AML, including the combination of HMA with venetoclax; response rates with this combination (up to 70%) appear impressively higher than historical data with HMA alone.25 The HMA/venetoclax combination was approved for patients who are aged ≥ 75 years or who have comorbidities that preclude the use of intensive induction chemotherapy, so its value has not formally been established in those who are fit for induction. However, the concept of “fit” vs “unfit” represents an attempt to dichotomize a continuum, with some patients inevitably being more “fit” than others. For patients who might previously have received 7+3 with borderline or questionable fitness, HMA/venetoclax now offers an approach with lower intensity and promising response rates that may be comparable to those with 7+3. Further data are needed to support the efficacy of this regimen; ultimately, a randomized trial would be the best approach to move the field forward.
Clinical case 1: part 2
The patient is taking 10 medications, which, based on the above, would increase her risk of negative outcomes. However, her functional status is excellent in that she was still working up until the time of diagnosis and is independent in all aspects of her life. Her Hematopoietic Cell Transplant Comorbidity Index (HCTCI) score is 1. An SPPB is performed, and the patient receives a score of 10. After discussion and counseling, the patient elects to pursue induction chemotherapy with 7+3.
AML induction: which risk factors are modifiable?
Although geriatric assessment may yield additional prognostic information, there are no data to suggest that patients who undergo these assessments have improved outcomes compared with those who do not. Future research should begin to address this question. However, as with any other negative prognostic factor, it must first be identified and confirmed before work can begin to determine whether it is modifiable or whether it should be used to influence therapy.
Once an older patient is receiving induction chemotherapy, can we intervene on functional limitations or other vulnerabilities to individualize care? Studies evaluating the effect of exercise during induction chemotherapy are ongoing. In a randomized controlled trial of a supervised exercise program during induction for patients of all ages, exercise was feasible and was associated with improved postchemotherapy aerobic fitness, lower extremity strength, and grip strength.26 Adherence was a limiting factor and was worse in older vs younger patients. Cognitive function was also improved in the exercise group, although this was a secondary end point. At present, it is reasonable to recommend regular exercise as tolerated for older patients receiving AML induction.
With respect to comorbidities, best practice would suggest maximizing the management of any existing medical problems and performing a review of medications to eliminate unnecessary ones. A recent study of 136 adults ≥60 years of age receiving intensive chemotherapy demonstrated that hyperglycemia and high glycemic variability were independently associated with lower probability of remission and inferior survival, even when controlling for the presence of diabetes.27 If validated, these findings would support a prospective trial of aggressive glycemic control, via dietary and/or pharmacologic intervention, for older adults receiving AML induction.
Clinical case 1: part 3
Patient 1 achieves a complete remission after induction chemotherapy with 7+3. Her course is complicated by Gram-negative sepsis, for which she requires 3 days in intensive care; however, she is left with no sequelae. During her induction, she has been HLA typed; her siblings have been typed as well, and one is a full match (age 70). A preliminary search in the unrelated donor database also yields >100 potential donors.
How to evaluate an older patient for alloHCT
alloHCT is increasingly being offered to older adults with hematologic malignancies. Trends over time represent improvements in nonmyeloablative conditioning regimens and supportive care, as well as an aging of the general population, with increased numbers of older patients who are then diagnosed with transplant-eligible diseases. Center for International Blood and Marrow Transplant Research (CIBMTR) data show that, in 2017, 31% of allogeneic transplants were performed in recipients aged ≥60 years, and 6% were in those aged ≥70 years; these numbers represent significant growth over the past decade.28 A more detailed look at 1106 patients ≥70 years of age receiving alloHCT between 2000 and 2013 has shown improvements in overall survival (OS) and progression-free survival (PFS) over time, although nonrelapse mortality (NRM) was not improved.29
The effect of chronologic age on transplant outcome remains somewhat controversial. In studies including patients of all ages, older age is associated with inferior NRM.30 However, in many studies focusing on older patients, age is not associated with posttransplant outcomes; for example, McClune et al reported on 1080 patients aged 40 to 79 years with AML in first remission or myelodysplastic syndrome; there was no impact of age on NRM or OS.31 This discrepancy may imply a limited additional prognostic impact of age once a patient is above a certain age threshold, and below which outcomes may, in fact, be better. Regardless of the explanation, most transplant centers believe that an evaluation for transplant should not be denied solely on the basis of chronologic age, at least up to the age of 75 years and possibly without an upper limit.
When evaluating an older patient for alloHCT, performance status and comorbidities are clearly part of the standard assessment, at any age. The majority of patients receiving alloHCT have a Karnofsky performance status (KPS) ≥ 80, making it a relatively coarse measure for prognostication. In the transplant setting, comorbidities are most commonly measured by the HCTCI, which has been widely validated. In a series of older transplant patients, the HCTCI and KPS were shown to be independently predictive of NRM and OS, although comorbidities were the stronger predictor.32 Whereas the HCTCI is undoubtedly important, it does have some limitations. One concern is its reliance on pulmonary function testing, which is the highest weighted comorbidity in the index (up to 3 points for this alone). The HCTCI was designed to include diffusing capacity of the lungs for carbon monoxide (DLCO), as calculated by the Dinkara equation; however, depending on the specific methodology that the pulmonary function laboratory uses to calculate DLCO (Cotes vs Dinkara), a patient may have significantly different results, leading to overestimation of comorbidity burden if the Cotes method is used.33 Secondly, the details of the comorbidities matter, even if the points assigned are the same; for example, a history of prostate cancer remotely resected is not equivalent to metastatic prostate cancer, although both would receive 3 points. Finally, there are many comorbidities not included in the HCTCI that might have an impact on the alloHCT decision, such as mild cognitive impairment, because of the effect that they may have on a patient’s functional abilities and independence.
In an effort to capture more of the heterogeneity of the older patient population, to better prognosticate beyond performance status and comorbidities, CGA has been studied in the allogeneic transplant setting.34-39 Although the details of the CGAs in these studies have differed in terms of specific instruments used to measure geriatric domains, some common themes are beginning to emerge. All studies have shown a significant degree of impairment in functional status and other geriatric domains in older patients determined fit for alloHCT, even in patients with excellent performance status and few comorbidities.40,41 In examining the effect of pretransplant CGA domains on posttransplant outcomes, functional status, as measured by IADL, and gait speed are associated with OS, although this was not consistent across all studies (Table 2). Work is in progress to validate the independent nature of these prognostic metrics, at the single-center level and in multicenter efforts. The upcoming CHARM study (BMT-CTN 1704) will evaluate the role of geriatric metrics in the prospective multicenter setting.
Studies evaluating the effect of pre-alloHCT geriatric assessment on post-alloHCT outcomes in older patients
| References | Patients | Geriatric measures associated with OS | Geriatric measures associated with NRM/TRM |
|---|---|---|---|
| Muffly et al34 | n = 203, age 50-73 y | Functional status (IADL), comorbidity (HCTCI), degree of inflammation (CRP), gait speed (15 ft), mental health (SF36-MCS; multivariate analysis). | Functional status (IADL), comorbidity (HCTCI), degree of inflammation (CRP). |
| Huang et al37 | n = 148, age 50-76 y | Functional status (IADL, MOS-PH) | Functional status (MOS-PH) |
| Deschler et al38 | n = 106, age 60-78 y | Gait speed (TUG test), fatigue. | Comorbidity (HCTCI) |
| References | Patients | Geriatric measures associated with OS | Geriatric measures associated with NRM/TRM |
|---|---|---|---|
| Muffly et al34 | n = 203, age 50-73 y | Functional status (IADL), comorbidity (HCTCI), degree of inflammation (CRP), gait speed (15 ft), mental health (SF36-MCS; multivariate analysis). | Functional status (IADL), comorbidity (HCTCI), degree of inflammation (CRP). |
| Huang et al37 | n = 148, age 50-76 y | Functional status (IADL, MOS-PH) | Functional status (MOS-PH) |
| Deschler et al38 | n = 106, age 60-78 y | Gait speed (TUG test), fatigue. | Comorbidity (HCTCI) |
CRP, C-reactive protein; MOS-PH, Medical Outcomes Study Physical Health scale; SF36-MCS, Mental Component Summary of the Medical Outcomes Short Form-36; TRM, treatment-related mortality; TUG, Timed Up and Go.
Other transplant-related considerations for the older patient
In addition to an evaluation of the patient’s ability to tolerate alloHCT, consideration must be given to donor options, disease control, and a patient’s preference for transplant vs alternative treatments. Available evidence suggests that, for patients aged ≥ 50 years with a good performance status, an older (≥50 years) sibling donor is associated with superior NRM, relapse risk, and OS compared with a younger (<50 years) unrelated donor.42 However, sibling donors aged 67+ years were associated with inferior outcomes compared with sibling donors aged 50 to 66 years. In this retrospective analysis, donors were all considered healthy enough for stem cell donation, but “healthy enough” was not prospectively defined; therefore, depending on the siblings’ health, choosing a younger well-matched unrelated donor may be reasonable.
Underlying disease control (including the presence of minimal residual disease) is an important predictor of posttransplant outcomes in patients of any age, but in older transplant recipients who are receiving reduced-intensity conditioning regimens, it is paramount. This is particularly true for patients with rapidly proliferative malignancies, such as AML. Finally, one must consider a patient’s treatment preferences for “high-risk high-reward” therapies, such as alloHCT, vs potentially life-prolonging approaches but with little to no possibility of cure.43
CGA: from assessment to plan
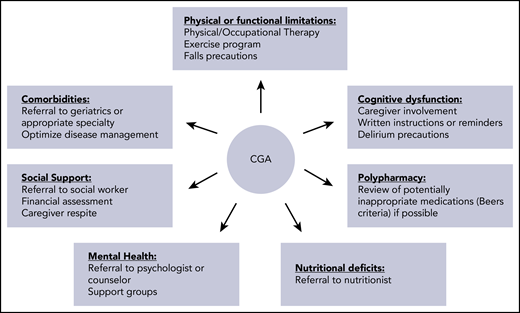
Although pretransplant CGA may be useful in prognosticating, our goal should not be to use it to exclude patients from transplant. Rather, we should aim to optimize any pretransplant vulnerabilities to maximize the number of patients who can safely and effectively receive alloHCT. At present, there is limited evidence that any pretransplant geriatric intervention can improve outcomes. Derman et al have recently shown that implementation of a CGA-guided interdisciplinary clinic to create an individualized care plan is associated with improved NRM and OS compared with historical outcomes prior to clinic implementation.44 Lin et al have also shown that peritransplant geriatric syndromes, specifically the occurrence of delirium or falls within the first 100 days, are associated with NRM and decreased OS, even when adjusting for other prognostic factors.45 Risk factors for delirium and falls in this study included history of falls, use of potentially inappropriate medications according to Beers criteria, impaired ADL, and age ≥ 70 years. Interventions to reduce the risk of delirium or falls could potentially improve outcomes, although this remains to be studied. Patients with functional limitations prior to alloHCT should be referred to physical therapy or other exercise programs; evidence suggests that improved functional capacity at transplant discharge is associated with better quality of life,46 supporting the concept of a personalized alloHCT inpatient exercise program.47 Finally, older patients should be monitored posttransplant for worsening function or emergence of new geriatric deficits. Older adults have worse physical well-being after alloHCT, are less likely to return to work, and, if chronic graft-versus-host disease is present, have increased probability of frailty.48,49 Referrals or other interventions may be needed posttransplant. My approach to the personalization of care for the older adult undergoing alloHCT is shown in Figure 2.
Clinical case 2: part 1
Patient 2 is a 76-year-old man with a history of diffuse large B-cell lymphoma. He was diagnosed with stage IV disease at presentation 1 year ago, with molecular testing consistent with germinal center B-cell like subtype. Testing for double-hit diffuse large B-cell lymphoma is negative. He was treated with RCHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone) every 3 weeks for 6 cycles. Unfortunately, his lymphoma has now relapsed, and he is started on salvage therapy with R-DHAOx (rituximab, dexamethasone, cytarabine and oxaliplatin). He presents for discussion of next steps in management, including whether he should have an autologous hematopoietic cell transplant (autoHCT).
His medical history is notable for nonvalvular atrial fibrillation and a small stroke 4 years ago, with some mild residual left leg weakness. He also has hypertension, hypercholesterolemia, and glaucoma. He takes 5 medications. He is retired, previously worked as a store manager, and lives alone.
How to evaluate an older patient for autoHCT
The most common indications for autoHCT are non-Hodgkin lymphoma (NHL) and multiple myeloma (MM).28 Because the preparative regimens for autoHCT for these diseases are different (multiagent chemotherapy vs single-agent melphalan), eligibility for autoHCT will differ depending on the indication.
In the context of MM, data from Europe have demonstrated increased numbers of autoHCT being performed in patients of all ages, but with the greatest increase in the population ≥65 years of age.50 Post-autoHCT survival also improved disproportionately in the older patient population. In a CIBMTR analysis, patients aged ≥70 years had NRM and PFS that were similar to younger patients; although 3-year OS was inferior in older patients, myeloma-specific mortality was similar.51 Therefore, most older patients with MM should be evaluated for transplant, regardless of chronologic age. However, it must be noted that the role of autoHCT for MM may continue to evolve in the face of novel therapeutic approaches incorporating daratumumab in the first-line setting (such as in the MAIA52 and Alcyone53 trials), particularly for older patients who are borderline autoHCT candidates and can now achieve excellent results with tolerable nontransplant approaches.
At a minimum, transplant evaluation for MM should include an assessment of performance status and comorbidities. In the above CIBMTR analysis, performance status remained an independent prognostic factor for OS, even when adjusting for age and comorbidities, with KPS < 80 and 80-90 both inferior to KPS 100.51 HCTCI of 0-1 vs 2+ was also independently associated with OS. Beyond performance status and comorbidities, some data now exist to support the use of geriatric assessment or individual geriatric metrics to determine fitness for autoHCT; previously, this was best studied in the transplant-ineligible MM population.54 In a study of 40 MM patients aged ≥65 years, CGA was performed at diagnosis and demonstrated significant rates of IADL dependence and polypharmacy, among others.55 Physician assessment of autoHCT eligibility correlated with age, comorbidities, performance status, and the Timed Up and Go test. Actual receipt of autoHCT correlated with age and IADL dependence. In a second study of 100 patients aged 36 to 75 years, CGA was performed prior to autoHCT.56 Physical function and ADL/IADL dependence were associated with transplant length of stay, and multiple geriatric measures predicted readmission risk. Weight loss was the only geriatric domain associated with event-free survival post-autoHCT. Finally, a third study examined 184 patients aged ≥50 years undergoing autoHCT, of whom 139 had MM or amyloid.57 Measures of patient-reported function, including IADL, patient-reported KPS, and the Functional Assessment of Cancer Therapy-Bone Marrow Transplant Physical subscale, were independently associated with OS and PFS, even after adjusting for age, provider-reported KPS, HCTCI, and disease status at transplant. At this time, given the totality of evidence, it seems reasonable to measure functional status pre-autoHCT in older patients with MM using IADL or another metric.
Another consideration for the older MM patient is selection of melphalan dose. In practice, many physicians reduce the dose of melphalan to ≤180 mg/m2 in older patients (commonly 140 mg/m2). Three recent registry studies have described the outcome of this practice.58-60 In general, there were few significant differences in posttransplant outcomes between melphalan 200 mg/m2 and lower doses. However, there were significant differences between groups in terms of age, creatinine, and other clinical features, making definitive conclusions difficult. There remains no standard approach to melphalan dose selection for the older patient, and randomized studies will be required to answer this question.
Unfortunately, in the context of NHL, there is a scarcity of data to guide the selection of older patients for autoHCT. Studies comparing outcomes of older vs younger patients are inconsistent but generally demonstrate inferior outcomes when the data set is large enough.61,62 Nonetheless, autoHCT is feasible in well-selected patients ≥70 years of age with NHL.63 In 1 series, a history of falls was associated with inferior NRM and OS.64
Clinical case 2: part 2
Patient 2 receives 2 cycles of R-DHAOx salvage chemotherapy but only achieves a partial response. During one of his hospitalizations, he has a fall. He is concerned about the toxicities associated with autoHCT and asks whether he should receive CAR T-cell therapy.
CAR T-cell therapy in the older adult
Given the relative novelty of this therapeutic approach, much less is known about the safety and efficacy of CAR T-cell therapy in older adults. Nonetheless, patients older than 70 years and even older than 80 years are receiving it in clinical practice, and the tolerance of cytokine release syndrome (CRS) and CAR-related encephalopathy syndrome (CRES) is a concern. A review of the trials leading to approval of 2 CAR T-cell products for NHL demonstrates that 20% to 25% of patients were ≥65 years of age, and there was no difference in efficacy in older vs younger patients.65,66 With respect to safety, the data are more uncertain. One study of 61 patients from a single center who received axicabtagene ciloleucel suggested that rates of CRS and CRES were similar in patients ≥65 years of age vs <65 years of age.67 However, a second report from the U.S. Food and Drug Administration combining data from 2 trials (N = 214) revealed similar rates of CRS in those ≥65 years of age but different rates of CRES manifestations.68 Rates of grade 3 or higher delirium and encephalopathy were higher in the older population (12% vs 2% and 35% vs 16%, respectively). Risk factors for CRES are not well defined and merit further study, particularly in patients ≥65 years of age.
Conclusions
The optimal approach to delivering intensive therapies to older adults with hematologic malignancies involves personalization. We are accustomed to the concept of personalized medicine in terms of therapies targeted at a tumor’s vulnerabilities, but we can also use this approach to address a patient’s vulnerabilities. In the last few years, increasing evidence suggests that geriatric assessment can provide meaningful information for prognostication in the setting of intensive leukemia induction and hematopoietic cell transplantation. Studies are ongoing to determine the best ways to adjust the care provided for those older patients with identified vulnerabilities to improve treatment tolerance and outcomes.
Authorship
Contribution: R.L.O. wrote the manuscript.
Conflict-of-interest disclosure: R.L.O. declares no competing financial interests. Off-label drug use: None disclosed.
Correspondence: Rebecca L. Olin, 400 Parnassus Ave, Box 0324, San Francisco, CA 94143; e-mail: rebecca.olin@ucsf.edu.
This article was selected by the Blood and Hematology 2019 American Society of Hematology Education Program editors for concurrent submission to Blood and Hematology 2019. It is reprinted in Hematology Am Soc Hematol Educ Program. 2019;2019:63-70.
