

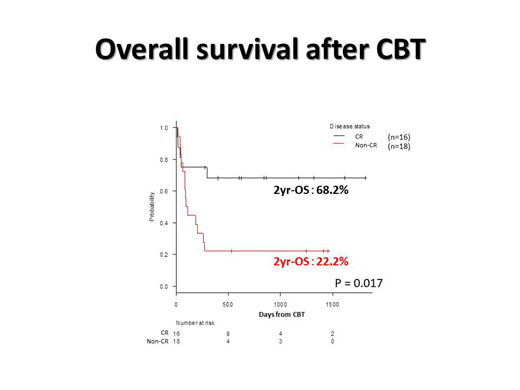
Adult T-cell leukemia/lymphoma (ATLL), which is a peripheral T-cell lymphoma related to human T-lymphotropic virus type I (HTLV-1), is known as a poor prognostic disease and its median age of onset is late 60s. Allogeneic hematopoietic stem cell transplantation is considered a treatment modality to contribute prolonging the survival in some population of patients. Although cord blood transplantation (CBT) widely practiced for hematological malignancies, a Japanese registry data suggested that 1 yr and 2 yrs overall survival (OS) after CBT in ATLL patients was only about 30% and 20%, respectively (Kato K, et al. 2014 BBMT). On the other hand, promising results were reported in the patients who were received CBT during their disease was controlled (Fukushima T, et al. 2013 IJH). Since it would be considered that CBT with non-TBI regimens, especially using reduced intensity conditioning (RIC), have a potential of engraftment failure compared to TBI regimen, it is less common conditioning regimen for CBT. Here we report a safety and an efficacy of CBT with non-TBI-RIC regimen using fludarabine (Flu) and melphalan (Mel) in 34 ATLL patients. We analyzed days from the beginning of systemic chemotherapy to transplantation, engraftment of neutrophil (EN), overall survival (OS), incidence of GVHD, non-relapse mortality (NRM) and disease-mortality (DRM), respectively. OS was defined as survival days from transplantation. OS were analyzed with logrank test. Cumulative incidence of EN and GVHD was considered with early death and NRM was considered with DRM as a competing risk. Incidence of GVHD, EN, NRM, and DRM was analyzed with Gray's method. Statistical significance defined P<0.05. Statistical analysis was carried out using the EZR. Thirty-four patients (18 male, 16 female) were consecutively undergone CBT with non-TBI-RIC regimen using Flu 125 mg/m2 and Mel 140 mg/m2 between January, 2014 and August, 2018 at our institute where is located in HTLV-1-endemic area. Twenty-eight patients used tacrolimus 0.02 mg /kg/day (TAC) and methotrexate (MTX) 5 mg/m2 / day at day 1, 3, 6 after transplantation, 5 patients TAC and mycophenolate mofetil (MMF) 750-2000 mg/day and one patient TAC alone as a GVHD prophylaxis. Median age at CBT was 61 years (44-70) and 30 patients were diagnosed as acute type ATLL whereas 4 lymphoma type. Sixteen patients were status in CR and 18 non-CR at CBT. Median duration of observation was 839.5 days (370-1890) and median time to CBT from the beginning of systemic chemotherapy was 113 days (61-416). Cumulative incidence of EN was 91.2 % and median time to EN was 20 days (14-68). OS at 2 years after transplantation (2 yr OS) was 43.9 %. 2 yr OS in CR patients was 68.2 % whereas 22.2 % in non-CR. There is no statistical significance about OS in age, gender, and incidence of GVHD. Cumulative incidence of NRM at day 100 and DRM at 1 year after CBT was 26.5 % and 26.5 %, respectively. CBT with non-TBI-RIC regimen using Flu/Mel was safe based on the result of feasible incidence of EN and NRM after CBT. Since 43.9 % of 2 yr OS was relatively high rate compared to previous report of Japanese registry data, CBT with non-TBI-RIC regimen using Flu/Mel can be a promising treatment strategy for ATLL.
Nakano:Novartis: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal