

Introduction
T-cell Lymphoblastic lymphoma (T-LBL) accounts for 90% of all LBLs, a rare and aggressive precursor lymphoblast originating hematological disorder. To date, there isn't any optimal prognostic model for T-LBL, which is a barrier to identify patients at high risk for relapse. Recent studies have shown that total metabolic tumor volume (TMTV) and total lesion glycolysis (TLG) measured on18F-fluorodeoxyglucose positron emission tomography-computed tomography (PET-CT) are useful prognostic parameters for in Hodgkin's lymphoma, diffuse large B cell lymphoma, and peripheral T cell lymphoma, etc. Here we discussed the prognostic role of these tumor burden indicators in T-LBL.
Methods
From January 2013 to December 2018, 37 newly diagnosed T-LBL patients with baseline PET-CT were included. The baseline maximum standardized uptake value (SUVmax) of all lesions was recorded, and the highest value was considered the SUVmax of the patient. Meanwhile, SUVmax of liver and mediastinum were obtained. The 41% SUVmax threshold method was used for MTV computation, TMTV was then obtained by summing the metabolic volumes of all local nodal and extra-nodal lesions. TLG was calculated as MTV multiply by average SUV. Progression-free survival (PFS) and overall survival (OS) were analyzed by Kaplan-Meier curves and compared by log-rank test. All statistical analyses were performed using SPSS version 25.0 software and P<0.05 was considered to be statistically significant.
Results
Among the 37 T-LBL patients included in the current study, the median age was 22 years with range from 12 to 75 years . 29 (78.4%) patients were male, and 32 (86.5%) of patients were in stage III and IV. 17 (45.9%) patients were given Hyper-CVAD/MA regimen, while 54.1% of these patients were treated with the modified BFM90 regimen. Detailed clinical characteristics for all patients were shown in Table 1.
The optimal cut-off values for SUVmax, TMTV and TLG were 12.7, 302cm3 and 890 respectively by ROC analysis. Patients with SUVmax≥12.7 were more likely to have advanced stage of disease, while patients with TMTV≥302cm3 or TLG≥890 were more inclined to have more than 2 sites of extra-nodal involvement.
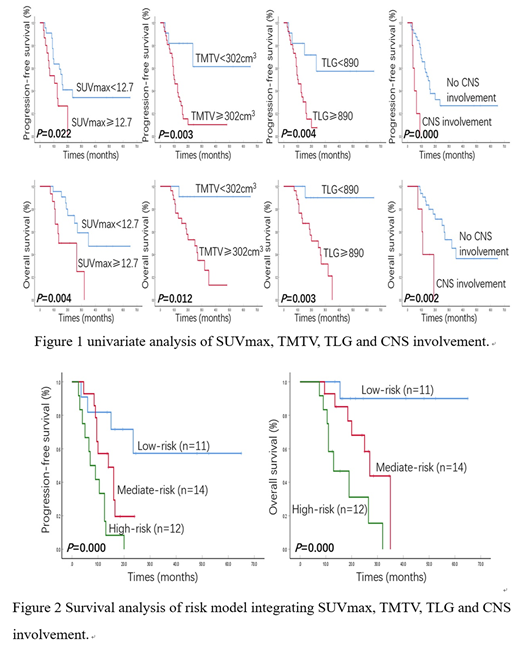
With a median follow-up time of 19 months (7.5-65 months), the estimated 4-year PFS and OS of the whole cohort was 23.3% and 32.2%, respectively. With a cutoff value of 12.7, the median PFS and OS were significantly shortened for patients with high SUVmax (PFS: 10.5 vs 16.0 months, P=0.022, OS: 13.5 vs 35.0 months, P=0.004, respectively). 3-year PFS were 10.3% in patients with TMTV<302cm3 and 61.4% in patients with TMTV≥302cm3 (P=0.003), while 3-year OS were 90.9% and 26.1%, respectively (P=0.012,). Similarly high TLG also indicated inferior PFS and OS (3 years PFS: 57.3% vs 7.6%, P=0.004, OS: 90.0% vs 31.6%, P=0.003, respectively). In addition, central nervous system (CNS) involvement was also found to be associated with shortened PFS and OS in the univariable test. Multivariable survival analysis demonstrated that TMTV≥302cm3 (HR=4.746, P=0.015), and CNS involvement (HR=5.309, P=0.006) were independent risk factors for PFS, while SUVmax≥12.7 (HR=3.170, P=0.035), TLG≥890 (HR=9.253, P=0.039) and CNS involvement (HR=5.880, P=0.007) were associated with worse OS independent of Ann Arbor stage, IPI score and treatment regimen.
Subsequently we integrated four independent prognostic factors SUVmax≥12.7, TMTV≥302cm3, TLG≥890 and CNS involvement to generate a risk model with each parameter ranking 1 score, which stratified the population into 3 risk groups: Group 1 (low-risk group), including patients who scored 0-1, had median PFS and OS of not reached at time of this study. Group 2 (mediate-risk group) including patients with score 2, had a median PFS of 14 months and median OS of 27 months. Group 3 (high-risk group) patients scored 3-4 with a median PFS of 7 months and OS of 13 months (Figure 2).
Conclusion
Baseline SUVmax , TMTV and TLG are strong predictors of outcome in T-LBL. In combination with CNS involvement, they are capable of identifying patients at high risk of early progression, which warrants further validation as a biomarker for development of first-line PET-CT adapted approaches in T-LBL.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal