

BACKGROUND: BMT recipients are vulnerable to accelerated atherosclerosis due to prior exposure to radiation with or without chemotherapy, and consequent long-term cardiovascular morbidity, such as stroke. A comprehensive evaluation of the risk of late-occurring stroke in adult BMT survivors and the associated risk factors has not been performed. We addressed this gap using the resources offered by the BMTSS.
METHODS: BMTSS includes patients transplanted between 1974 and 2014 at 3 US sites who survived ≥2y after BMT, were alive and ≥18y at BMTSS survey completion. The survey asked participants to report if a healthcare provider had diagnosed specific chronic health conditions (including stroke), or relapse of primary cancer or development of new cancer, along with age at diagnosis. The participants provided information on sociodemographics, health behaviors and medication use. Medical record abstraction was used for information regarding primary cancer diagnosis, therapeutic exposures (pre-BMT chemotherapy/radiation, transplant preparative regimens), stem cell source (autologous, allogeneic), graft type (bone marrow, cord blood or peripheral blood stem cells), and history of chronic graft vs. host disease (GvHD). A cohort of 908 siblings also completed the BMTSS survey and served as a comparison group. Informed consent was obtained from all participants.
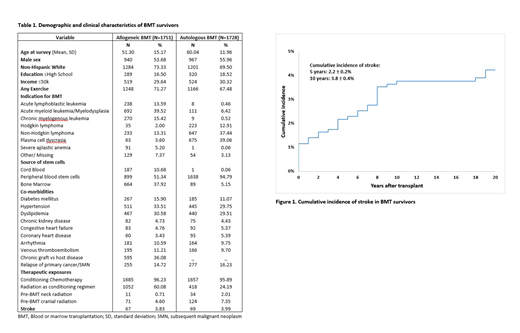
RESULTS: The study included 3,479 BMT survivors; 50.3% had received an allogeneic BMT, 54.8% were males; 71.4% were non-Hispanic whites. Median age at study participation was 59y (range: 18-89y) for BMT survivors and 57y (range: 18-90y) for siblings. Patient characteristics are shown in Table 1. BMT survivors were followed for a median of 9y (range: 2-41 y) from BMT. Stroke was reported by 136 BMT survivors (67 allogeneic, 69 autologous); of these, 75 (55%) patients developed stroke ≥2y after BMT. Conditional on surviving ≥2y after BMT, the 10y cumulative incidence of stroke was 3.8% (Fig 1), and was comparable for allogeneic (3.4±0.5%) and autologous (4.2±0.6%) BMT recipients, p=0.3.
Stroke in BMT recipients compared with siblings: Using logistic regression, and after adjusting for sociodemographics, physical activity and relevant comorbidities, we found that allogeneic BMT survivors were at a 2.1-fold higher odds of reporting stroke as compared to siblings (95%CI: 1.2-3.7, p=0.01), and autologous BMT recipients were at a 1.7-fold higher odds of reporting stroke compared to siblings (95%CI: 0.9-3.0, p=0.09).
Stroke after Allogeneic BMT: History of hypertension (HR=2.2, 95%CI: 1.2-3.9, p=0.007), venous thromboembolism (HR=3.4, 95%CI: 1.6-7.1, p=0.002), diagnosis of acute lymphoblastic leukemia (HR=4.9, 95%CI: 1.6-15.0, p=0.006), acute myeloid leukemia/ myelodysplastic syndrome (HR=5.2, 95%CI: 1.4-19.0, p=0.013) (ref: non Hodgkin lymphoma), pre-BMT exposure to alkylating agents (HR=3.3, 95%CI: 1.3-8.5, p=0.01) and pre-BMT neck radiation (HR=5.4, 95%CI: 1.2-23.8, p=0.03) were associated with increased stroke risk. Exercise was associated with lower stroke risk (HR: 0.5, 95%CI: 0.3-0.9, p=0.01).
Stroke after Autologous BMT: The risk factors for stroke in autologous BMT survivors included: increasing age at BMT (HR=1.02/y, 95%CI: 1.0-1.1, p=0.05), history of hypertension (HR=1.8, 95%CI: 1.1-3.2, p=0.03), coronary heart disease (HR=2.8, 95%CI: 1.3-6.4, p=0.01) and venous thromboembolism (HR=2.3, 95%CI: 1.1-4.7, p=0.02).
Relapse of primary disease or development of new cancer were not associated with increased stroke risk in either autologous or allogeneic BMT recipients.
CONCLUSION: In this large study, we found that the incidence of stroke was 4% among BMT survivors, and that they are at an increased risk of developing stroke when compared to an unaffected comparison group. The study also identified subgroups among BMT survivors at increased risk of stroke such as those who received neck radiation and those with cardiovascular comorbidity. These findings suggest a need for increased awareness of stroke as a late complication of BMT, such that aggressive management of cardiovascular risk factors can be instituted among those at highest risk.
Weisdorf:Incyte: Research Funding; Fate Therapeutics: Consultancy; Pharmacyclics: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal