

Background: Recombinant and synthetic adeno-associated virus (AAV) vectors are in development for gene transfer in patients with hemophilia A (HA) or hemophilia B (HB). These include liver-directed recombinant AAV8 vectors BAX 888/SHP654/TAK-754 factor VIII (FVIII) gene therapy (GT) for severe HA, and SHP648/TAK-748 factor IX (FIX) GT for HB (Baxalta US Inc., a Takeda company, Lexington, MA, USA). However, environmental exposure to wild-type AAVs can result in individuals developing antibodies and cell-mediated immune responses to the naturally occurring AAV. While natural exposure to AAV does not result in any known disease in humans, presence of preexisting immunity can block delivery and prevent sustained expression of the transgene by an AAV-based vector in a gene therapy setting. Of the AAV serotypes, AAV2 is the most frequently encountered natural human infection and AAV5 and AAV8 have been the most commonly used vectors for hemophilia GT. Therefore, it is important to assess the prevalence and co-prevalence of antibody and T cell-mediated responses against each of these AAV serotypes and to better characterize the association between humoral and cellular immunity in people with hemophilia.
Aims: To determine the prevalence of preexisting antibody-mediated immunity against AAV2, AAV5 and AAV8 and the association between AAV8-specific humoral and cell-mediated responses in adult patients with HA and HB in an international prospective, epidemiological study.
Methods: This ongoing seroprevalence study involved adult male patients (18-75 years of age) with severe HA (<1% plasma FVIII activity) or severe/moderate HB (≤2% plasma FIX activity) recruited from hemophilia treatment centers in the United States and Europe (NCT03185897). Participants consented to collection of peripheral blood at either a single or multiple annual outpatient study visits, in order to explore fluctuations of the immune response over time. Local ethics committee approval was obtained. Titers for anti-AAV2, anti-AAV5 and anti-AAV8 neutralizing antibodies (NAbs) were determined using a cell-based transduction inhibition assay, with seropositivity defined as a titer ≥1:5. Titers for anti-AAV2, anti-AAV5 and anti-AAV8 binding antibodies (BAbs) were quantitated by indirect enzyme-linked immunosorbent assay (ELISA), with seropositivity defined as a titer ≥1:80. Cell-mediated immune responses to AAV8 peptide antigens were measured in peripheral blood mononuclear cells using an interferon-γ enzyme-linked immunospot (ELISpot) assay. Samples with a signal ≥3 times background and >60 spots per million cells were defined as positive.
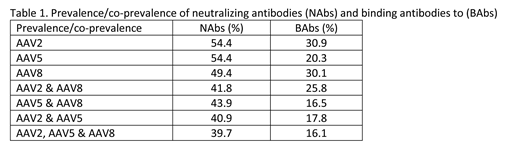
Results: Here we present data from patients who completed at least a single visit at the time of the interim, one year data cut (November 9, 2018). Of 242 patients enrolled (mean ± SD age: 35.3 ± 11.4 years), 194 patients had HA and 48 patients had HB. The overall co-prevalence of NAbs and BAbs to AAV2, AAV5 and AAV8 was 39.7% (HA: 38.1%, 72/189; HB: 45.8%, 22/48) and 16.1% (HA: 16.5%, 31/188; HB: 14.6%, 7/48) respectively, with further details shown in Table 1. Overall, 38.3% of patients (82/214) exhibited a T cell-mediated immune response to AAV8 peptide antigens (HA: 35.9%, 61/170; HB: 47.7%, 21/44). Among patients with AAV-8-specific NAbs, 37.9% (39/103) demonstrated positive AAV8-specific ELISPOT results. (HA: 35.7%, 30/84; HB: 47.4%, 9/19).
Conclusion: The findings from this ongoing study demonstrate that approximately 50% of patients with hemophilia have preexistent NAb responses to AAV2, AAV5 or AAV8 with 40% demonstrating co-prevalence to all 3 evaluated AAV serotypes. Similar percentages of patients exhibited a positive cellular response to AAV8 antigens. Further, patients with HB demonstrated a slightly higher co-prevalence and a higher cellular response than patients with HA. In the combined HA and HB cohorts, co-prevalence was almost 40% for AAV8-specific humoral and T-cell mediated immunity. These data will add to our appreciation of preexisting AAV immunity that prevent patient participation in gene therapy trials.
Rajavel:Baxalta US Inc., a Takeda company: Employment, Equity Ownership. Ayash-Rashkovsky:Baxalta US Inc., a Takeda company: Employment, Equity Ownership. Tang:Baxalta US Inc., a Takeda company: Employment, Equity Ownership. Gangadharan:Baxalta Innovations GmbH, a Takeda company: Employment. de la Rosa:Baxalta Innovations GmbH, a Takeda company: Employment. Ewenstein:Baxalta US Inc., a Takeda company: Employment, Equity Ownership, Other: a Takeda stock owner.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal