

Background. Anaplastic lymphoma kinase positive systemic anaplastic large cell lymphoma (ALK+ ALCL) represents an aggressive T-cell malignancy that primarily affects children and younger adults. Upon treatment with CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) or CHOP-like regimens its prognosis is relatively favourable compared to other aggressive T-cell lymphomas, however, the rare event of disease reoccurrence remains particularly challenging. ALCL is CD30 positive, and mono treatment with brentuximab vedotin (BrV) can achieve long term remissions in only few relapsed patients not receiving consolidating stem cell transplantation (Pro B. et al. Blood 2017). A subset of ALCL patients express platelet derived growth factor receptor (PDGFR) alpha or beta in their tumour cells which is induced by ALK via AP-1 transcription factor activation. We previously demonstrated that PDGFR blockade by the Abl/c-Kit/PDGFR kinase inhibitor imatinib is an effective treatment concept for ALK+ ALCL in experimental mouse models (Laimer D. et al. Nature Med. 2012). Here we aimed to assess the prognostic value of PDGFR expression and to probe the clinical value of its targeting by imatinib in ALK+ ALCL patients.
Methods. The impact of PDGFR expression to predict clinical outcome was analyzed in samples of 98 ALK+ ALCL patients included in the studies NHL-BFM 90, 95 and ALCL99 between 1992 and 2006. Six patients (age 18-45) with chemo-refractory ALK+ ALCL were prospectively treated with imatinib plus (4) or minus (2) BrV. 33% (2/6) had previously received salvage treatment with stem cell transplantation (SCT). Three of the patients had been enrolled in a prospective single-arm study combining imatinib and BrV, a trial that was terminated due to poor patient recruitment (AGMT ALCL1 trial, EudraCT No.: 2013-003505-26, supported by Takeda®). PDGFR alpha and beta expression analyses were performed on tumour samples of treated patients.
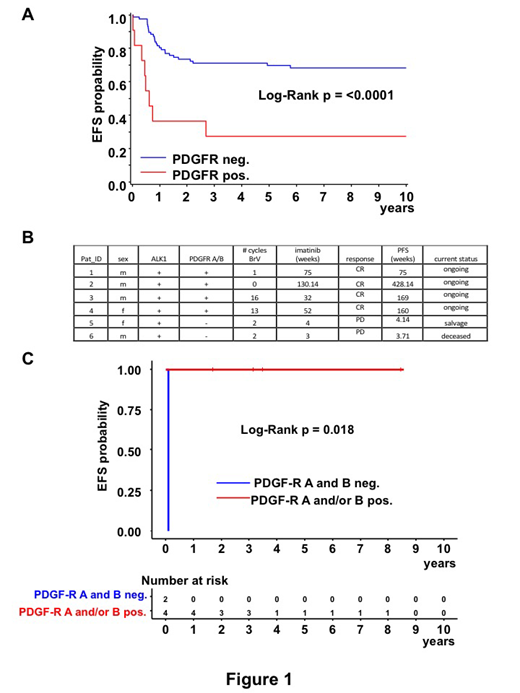
Results. ALK+ ALCL patients with high PDGFR expression on tumor cells (n=11) had a significantly lower event-free survival rate (EFS) at 5 years compared to patients with no or low expression (n=87) (27±13% versus 70±5%, respectively, p<0.001, figure 1a). Four of the six patients with relapsed/ refractory ALK+ ALCL responded to imatinib +/- BrV with a rapid metabolic complete remission (CR). At a median clinical follow-up of 52 months (range 20 to108) all responding patients demonstrated an ongoing CR without SCT even after imatinib was discontinued with an average time on imatinib of 49 weeks (range 32 to 130; figure 1b). Half (2/4) of responding patients received no or only 1 infusion of BrV; both non-responding patients had received BrV. Importantly, despite the few patients that could be prospectively treated, PDGFR expression status had a significant impact on clinical course. All patients (4/4) who expressed either PDGFR alpha or beta in tumour cells and in the lymph node microenvironment responded with an ongoing metabolic CR, whereas the two patients whose lymphoma cells had negative PDGFR expression failed to respond (EFS: 4 versus 210 weeks, p = 0.018; figure 1c).
Conclusions. 1) PDGFR expression is a poor risk factor in ALK+ ALCL. 2) Imatinib alone or in combination with BrV overcomes chemo-resistance conferred by PDGFR expression. 3) Imatinib treatment can be discontinued with ongoing CR. 4) These observations suggest that PDGFR expressing ALK+ ALCL patients might benefit from early treatment with imatinib.
Staber:Takeda-Millenium: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Janssen: Honoraria, Speakers Bureau; MSD: Honoraria, Speakers Bureau; Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees. Klapper:Roche, Takeda, Amgen, Regeneron: Honoraria, Research Funding. Mayerhoefer:Siemens: Research Funding, Speakers Bureau; BMS: Speakers Bureau. Greil:Gilead: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Pfizer: Honoraria, Research Funding; Ratiopharm: Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Eisai: Honoraria; Genentech: Honoraria, Research Funding; Janssen-Cilag: Honoraria; GSK: Research Funding; Sandoz: Honoraria; Roche: Consultancy, Honoraria, Research Funding; Daiichi Sankyo: Consultancy, Honoraria; MSD: Consultancy, Honoraria, Research Funding; Merck: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; Sanofi Aventis: Honoraria; Boehringer Ingelheim: Honoraria; Mundipharma: Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding. Jaeger:Novartis, Roche, Sandoz: Consultancy; AbbVie, Celgene, Gilead, Novartis, Roche, Takeda Millennium: Research Funding; Amgen, AbbVie, Celgene, Eisai, Gilead, Janssen, Novartis, Roche, Takeda Millennium, MSD, BMS, Sanofi: Honoraria; Celgene, Roche, Janssen, Gilead, Novartis, MSD, AbbVie, Sanofi: Membership on an entity's Board of Directors or advisory committees.
Imatinib - bcr-abl Inhibitor

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal