

Background
PT-Cy has emerged as an effective strategy for graft-versus-host disease (GVHD) prophylaxis in Haplo. The reported risk of GVHD with non-PT-Cy in pts receiving MUDs varies between centers. In this report, we compared the engraftment rates, survival, risk of GVHD and comorbidities between PT-Cy Haplo and r-ATG-based MUDs approach in pts with relapse/refractory lymphoma receiving an allogeneic transplantation.
Method
We retrospectively evaluated 160 adult pts with lymphoma who received Haplo (n=35) or r-ATG-MUDs (n=125) at our center between 2012 and 2018. Pts received GVHD prophylaxis of r-ATG (2-4 mg/kg total on days -3 to -1), tacrolimus and methotrexate if MUD, and tacrolimus and mycophenolate mofetil in addition to PT-Cy (50 mg/kg on days+3, +4) if Haplo. Tacrolimus taper was initiated at 6 months after transplantation in pts with no active GVHD. The study was IRB-approved.
Results
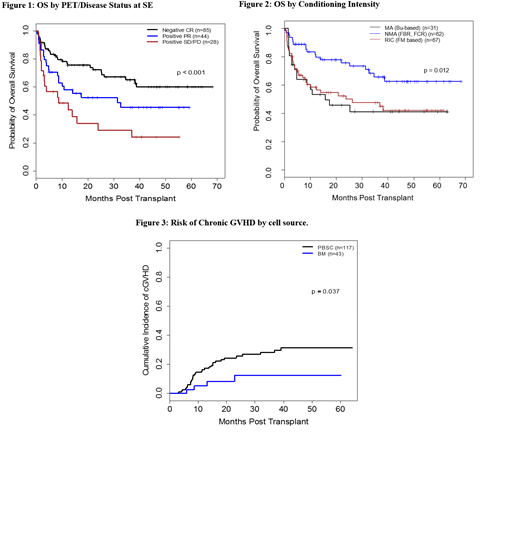
Haplo pts were more likely to be younger (median age 47 vs 55 yrs; P=0.032), have a lower HCT-Comorbidity Index (median 2 vs 3; P=0.048), and to include more diffuse large b-cell lymphoma (31% vs 22%, and Hodgkins disease (29% vs 16%) (P=0.015). Significant differences were also observed in the conditioning intensity and cell source of transplants between the 2 groups. The majority of Haplo pts (80%) received a reduced intensity-conditioning (RIC) of melphalan/fludarabine +/- 2Gy TBI; the remaining received a myeloablative (MA) busulfan-based regimen (9%) or nonmyeloablative (NMA) (11%) conditioning. In comparison, the percentage of MUDs pts receiving RIC, MA and NMA [bendamustine, fludarabine, rituximab or fludarabine, cyclophophamide, rituximab were 31%, 22% and 46%, respectively (P<0.001). The percentage of pts receiving bone marrow as a source of cells in the Haplo and MUDs groups were 74% vs 14%, respectively (P<0.001). There was no difference in the # of prior therapies received (median = 3, in both), the # of pts who failed a prior autologous (37% vs 26%; P=0.21), disease status (CR vs PR vs refractory; P=0.3), IPI >2 (25% vs 19%, P=0.73) or PET-positive status (55% vs 44%, P=0.33) at study entry between the 2 groups. PT-Cy Halplo group had a significantly higher incidence of symptomatic BK- induced hemorrhagic cystitis compared to r-ATG MUD group (49% vs 10%, P< 0.001). Delayed engraftment was noted in PT-Cy Haplo group compared to r-ATG MUD group with median time to achieve ANC > 500 (18 days vs 10 days; P<0.001), and platelets > 20k were 25.5 days vs 10 days (P<0.001), respectively. The median follow-up time for pts treated with PT-Cy Haplo and r-ATG MUD pts was 12.1 and 20.8 months, respectively. Similar survival and non-relapse mortality (NRM) rates were observed between the 2 groups. The 1-year OS rates were 64% vs 67% (P=0.76) and the 1-year PFS rates were 52% vs 58% (P=0.67). The cumulative incidence (CI) of 1-year NRM was 30% vs 26%, respectively (P=0.66). Chemo-sensitivity (Figure 1), NMA conditioning (Figure 2), and HCT-Comorbidity Index of < 4 were associated with a better OS and PFS in univariate and multivariable analyses. Among histologies, pts with follicular lymphomas had the best OS and PFS. T-cell lymphoma had the worse outcomes. In addition, cystitis was associated with a lower survival rate by univariate analysis (P=0.036). The CI of acute 2-4 GVHD (26% vs 33%, P=0.43), acute 3-4 GVHD (14% vs 12%, P=0.66), and 1-year CI of chronic GVHD (6% vs 15%, P=0.19) were not statistically different between PT-Cy Haplo and r-ATG MUD. By univariate analysis, bone marrow source of graft was the only factor that was found to be significantly associated with a lower risk of chronic GVHD (HR 0.34; P=0.041) (Figure 3).
Conclusion
Our data show similar survival rates and risk of acute and chronic GVHD in pts with lymphoma who received PT-Cy Haplo and r-ATG MUD. The use of bone marrow graft was the only predictor of a lower incidence of chronic GVHD. Considering the statistically significant delayed time to engraftment and the higher risk of hemorrhagic cystitis, a MUD remains the donor of choice in lymphoma pts who have this option.
Jabbour:Takeda: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Adaptive: Consultancy, Research Funding; Cyclacel LTD: Research Funding; AbbVie: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; BMS: Consultancy, Research Funding. Bashir:Imbrium: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Spectrum: Membership on an entity's Board of Directors or advisory committees; Kite: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding; StemLine: Research Funding; Acrotech: Research Funding; Celgene: Research Funding. Oran:Astex pharmaceuticals: Research Funding; AROG pharmaceuticals: Research Funding. Kebriaei:Kite: Honoraria; Amgen: Research Funding; Jazz: Consultancy; Pfizer: Honoraria. Popat:Bayer: Research Funding; Incyte: Research Funding; Jazz: Consultancy. Champlin:Johnson and Johnson: Consultancy; Sanofi-Genzyme: Research Funding; Actinium: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal