

Introduction
The combination of anti-thymoglobulin (ATG), post-transplant cyclophosphamide (PTCy) and cyclosporine (CsA) provides an effective control of graft-versus host disease (GVHD) in allo-HSCT using peripheral blood stem cell (PBSC) grafts, as has been reported by Dr. Viswabandya et al.
We aim to report a large, single center experience in reduced intensity conditioning (RIC) allo-HSCT using dual T-cell depletion with ATG and PTCy combined with CsA for GVHD prophylaxis using grafts from 10/10 matched unrelated donors.
Patients and methods
Between October 2015 and April 2019, 167 adult patients diagnosed with hematological malignancies underwent first 10/10 MUD RIC allo-HSCT. RIC regimen was composed by fludarabine, busulfan, and 200cGy of total body irradiation. For GVHD prophylaxis all recipients received rabbit-ATG, PTCy 50mg/m2/day on day +3 and +4, and CsA since day +5.
One hundred sixteen (69.5%) recipients, transplanted between 2015 and May 2018, received a total dose of 4.5mg/kg of rabbit-ATG (given on day -3,-2 and -1). In May 2018, the dose of ATG was lowered to a total of 2mg/kg (given on day -3 and -2). A total of 51 (30.5%) recipients received the lowered dose of ATG.
The median follow-up of the entire cohort was 14 months (range: 0.4-44.5). For those patients who got a higher dose of ATG was 20 months and for those who received a lower dose of ATG was 8.8 months.
Data was collected retrospectively and updated on July 2019. Cumulative incidence (Cum.Inc) of GVHD analysis was assessed accounting relapse and death as competing events.
Results
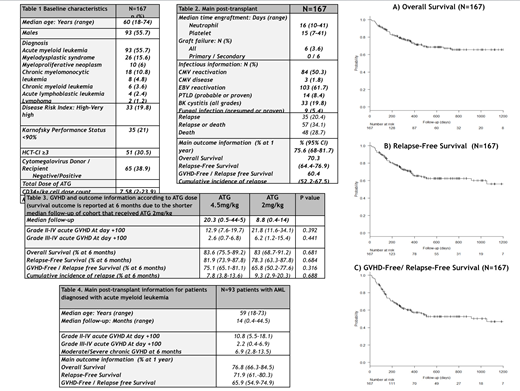
Baseline and post-transplant information are summarized in the Table 1 and 2. Ninety-three (55.7%) recipients were diagnosed with acute myeloid leukemia (AML).
The cum.Inc of grade II-IV and grade III-IV acute GVHD at day +100 was respectively 15.6% (95% confidence interval (CI) 10.6-21.6) and 3.6% (95% CI 1.5-7.3). The cum.Inc of acute GVHD was not significantly affected by the dose of ATG (P>0.05). The cum.Inc of chronic GVHD was 10.9% (95% CI 6.6-16.4). Due to the shorter median follow up of the cohort that received a lower dose of ATG, the impact of the reduction of the dose in the cum.Inc of chronic GVHD was not explored.
Overall, 48 (28.7%) recipients died and 35 (20.4%) relapsed. Main causes of death were relapse (14.4%) and infection (9.6%). Outcome information is reported in the Table 2 and Plot A, B and C. One-year overall survival (OS), relapse-free survival (RFS) and GVHD-free/RFS (GFRFS) were respectively 75.6%, 70.3%, 60.4%.
Table 3 summarizes the impact of the use of a different dose of ATG in acute GVHD and post-transplant outcome. No significant differences were found between the two groups that receive a different dose of ATG. However, median follow-up was shorter in the cohort that received 2mg/kg of ATG.
Table 4 reports the main post-allo-HSCT information of patients diagnosed with AML. One-year OS, RFS and GRFRS for this subgroup of patients were 76.8%, 71.9% and 65.9%.
Conclusion
The unique and modern combination of RIC PB allo-HSCT using ATG, PTCY and CsA for GVHD prophylaxis results in impressive post-transplant outcomes using 10/10 MUD.
The use of dual T-cell depletion with ATG and PTCy is safe and provides an extraordinary control of GVHD with acceptable relapse rates using PB stem cell 10/10 MUD grafts.
ATG of only 2mg/kg when it is combined with PTCy and CsA, results in an effective control of acute GVHD rates. The optimal dose of ATG for GVHD prophylaxis is not well established. Further investigations need to be done to determine the efficacy of a lower dose of ATG controlling chronic GVHD in this setting.
For patients diagnosed with AML, this protocol is safe and an effective approach when a 10/10 MUD is available.
Michelis:CSL Behring: Other: Financial Support. Mattsson:Celgene: Honoraria; Gilead: Honoraria; Therakos: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal