

Background
Stroke is one of the leading causes of death in the United States and carries a significant risk of morbidity and mortality. P2Y12 inhibitors (Clopidogrel, Ticagrelor etc.) as monotherapy or in combination are used to decrease risk of future ischemic strokes. While standard dosing regimens are currently being used ,the effect of obesity on their efficacy remains unclear. We examined the effect of obesity on the efficacy of P2Y12 inhibitors compared to controls in preventing future incidence of ischemic stroke.
Methods
We conducted a systematic search on Pubmed, Embase, Cochrane Library, Cochrane Central Register of Controlled Trials and Web of Science to identify relevant randomized clinicals (RCTs) until 31st, July 2019. Our primary outcome of interest was to assess the efficacy of P2Y12 inhibitors (Clopidogrel and Ticagrelor) in preventing recurrent stroke among obese patients with recent stroke or obese individuals at high risk for atherothrombotic events. Obesity was defined as body mass index (BMI) >30kg/m2 and normal BMI was defined as 18 kg/m2 to 25kg/m2. Collected data included dosing regimens, hazard ratio (HR) and confidence interval (CI) for primary outcome in each study arm. We used DerSimonian and Laird random-effects model to estimate pooled HR along with 95% CI using Comprehensive Meta Analysis (CMA) version 3.3. We also performed a sensitivity analysis of the RCTs using Clopidogrel. Heterogeneity was assessed using I2 statistic (<25%=negligible, 25% to 50%= moderate, ≥70% =substantial). Publication bias was assessed using funnel plot and risk of bias was assessed using Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool for clinical trials.
Results
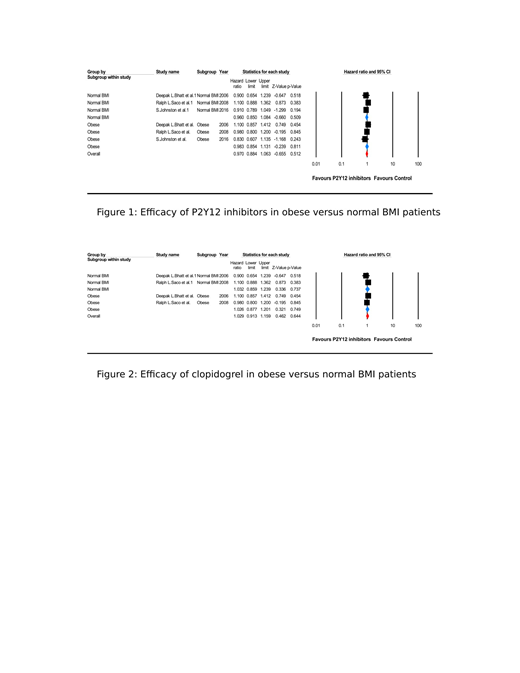
Out of 2142 studies initially retrieved, we included three RCTS (n=49134) namely CHARISMA (clopidogrel (Clopi) plus asprin (ASA) vs ASA), PRoFESS (Clopi vs ASA plus dipyridamole (Dipy), and SOCRATES (ticagrelor (Tica) vs ASA). There was no statistical difference in the efficacy of P2Y12 inhibitors in preventing stroke when obese and normal BMI patients were compared (p-value of interaction = 0.80, HR: 0.97 [95% CI: 0.88-1.06]) (figure 1). Sensitivity analysis of patients using Clopi also revealed no statistical difference in preventing future stroke (p-value of interaction = 0.96, HR: 1.03 [95% CI: 0.91-1.16]) (figure 2) in obese vs normal BMI patients. Moreover, there was no difference in the efficacy of P2Y12 inhibitors vs control arm (HR: 0.98 [95% CI: 0.85-1.13], p-value: 0.81, I2=0%) and Clopidogrel only vs Control arm (HR: 1.03 [95% CI: 0.88-1.20], p-value: 0.75, I2=0%) in preventing stroke among obese patients.
Conclusion
Although Obesity is a known risk factor for cardiovascular events including stroke, and it affects the metabolism of many drugs including anticoagulants among others which was the basis of the idea to look into the published literature on the topic in an attempt to find a correlation between obesity and an increased risk of stroke in patients on P2Y12 inhibitors, there was no difference in the efficacy of standard dose P2Y12 inhibitors in obese patients as compared to normal BMI patients. Sensitivity analysis of trials using standard dose Clopidogrel also revealed no statistical difference, we believe the topic might benefit from further studies .
Anwer:Seattle Genetics: Membership on an entity's Board of Directors or advisory committees; In-Cyte: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal