

Background
The pneumatic tube delivery system (PTDS) has been an integral part of blood bank (BB) operations at our institution ever since its implementation in the early 2000s. Its reliable performance is essential for rapid and accurate delivery of blood products, impacting patient safety and product integrity. However, malfunctioning operational events are not uncommon given PTDS complexity and hospital-wide utilization. In 2018, 33 of 285 (12%) blood products were wasted due to PTDS events at our institution. Here we review the root cause analysis (RCA) of a patient safety event involving delayed transfusions and a wasted blood product causing temporary harm to two patients.
Methods
Two patients, both hospitalized on the same floor, simultaneously experienced significant delays in red blood cell (RBC) transfusions. One patient with active bleeding experienced a 2-hour delay and another patient with anemia experienced a 50-minute delay before appropriate transfusion occurred. The two patients did not receive their transfusions until their nurses physically retrieved RBC units from the BB. An incident report was filed by a floor nurse, which prompted a RCA involving the laboratory quality and patient safety team, the BB, the hospital maintenance department overseeing the PTDS, and the information systems service controlling programming of the PTDS.
Results
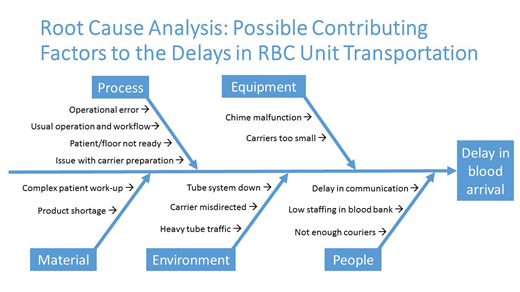
Operational challenges surrounding the PTDS were central to the multiple root causes identified (see Table). RBC units sent to the floor from the BB were electronically directed to another floor or returned to the BB, which resulted in a waste of one RBC unit. Despite multiple potential contributing factors identified, deeper investigation did not uncover evidence for any specific root cause and the electronic tube transaction history showed normal PTDS operations during the time of the incident, with all transactions appearing as successfully completed within expected timeframes. Neither of the patients involved in this safety event experienced permanent harm. The findings of this investigation were reviewed at our departmental Pathology Morbidity and Mortality conference together with stakeholders from hospital maintenance.
Conclusion
The root causes for PTDS technical malfunctioning leading to this safety event remain uncertain despite a collaborative RCA. This multidisciplinary retrospective RCA process, however, provided an opportunity for greater awareness of the complex mechanism of the PTDS, promoted awareness of the roles of the various stakeholders involved, and fostered interdepartmental collaboration to prevent future patient safety incidents using quality improvement principles.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal