

Background
MDS is a heterogeneous disease and the revised International Prognostic Scoring System (IPSS-R) is utilized in prognostication. The percentage (%) of blasts in the bone marrow is determined in the aspirate morphologically. Though the former is the standard of care the blast percentage is also reported by flow cytometry and biopsy which can many times be inconsistent. We previously presented the utilization of biopsy based blast percentage which showed meaningful prognostic groups compared to aspirate. In this study we compare the blasts as reported by the aspirate and flow cytometry in MDS-EB in calculating IPSS-R.
Methods
The MDS database was reviewed for cases of MDS-EB after due IRB approval at the Mayo clinic. We calculated IPSS-R scores based on the aspirate blast % (IPSS-RAsp) and flow blast% (IPSS-Rfl). The aspirate blast percentage was reported morphologically. Suboptimal aspirates were excluded from the study. The flow blast percentage was determined by immunophenotyping. The overall survival (OS) was determined by IPSS-RAsp and IPSS-RFl. OS estimates were calculated by Kaplan-Meier curves and log-rank testing using JMP v.13. Uno's concordance statistic was used to compare the 2 risk scoring systems.
Results
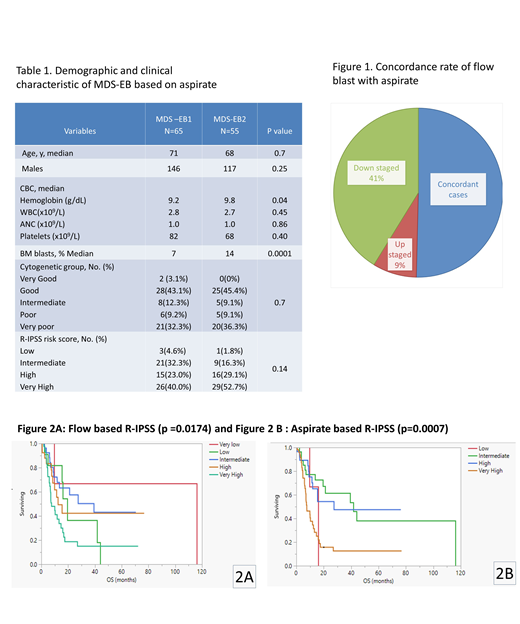
Of 1322 patients, 431 (33%) cases were identified with MDS-EB out of which 120 (29%) cases had blasts reported in the aspirate and flow. Based on aspirate MDS EB1: 54% (n=65), MDS EB2 46% (n=55). The hematological, cytogenetic and R-IPSS categories were compared between MDS-EB1 and MDS- EB 2. The blast percentage and hemoglobin levels was significantly different between MDS-EB1 and EB2 as seen in table 1, however the IPSS-R risk groups were not significantly different.
The flow cytometry was concordant with aspirate in 66/120 (55%) cases. Out of the dis-concordant cases only 20% (11/54) was upstaged by flow cytometry with most of the patients being down staged as expected by the techniques used in processing the blood and hence not reliable when reported low (Figure 1). The OS outcomes based on the IPSS- R asp, IPSS-Rfl areshown in figure 2A,2B .The p value with aspirate based R-IPSS was more significant than flow cytometry based R-IPSS (p= 0.0007 vs 0.0174). We compared the two models for observed OS differences using the Uno model which was not statistically significant. (p= 0.6)
Conclusions
Both models did not show a difference which is likely due to the very small sample size. However flow cytometry did down stage more patients when disconcordant and may have less value in that setting. It would be ideal to compare all 3 models aspirate, biopsy and flow cytometry however we did not have enough number of patients to do the comparison.
Patnaik:Stem Line Pharmaceuticals.: Membership on an entity's Board of Directors or advisory committees. Al-Kali:Astex Pharmaceuticals, Inc.: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal