

Background: Patients with multiple myeloma are frequently treated with bortezomib, a proteasome inhibitor, which is associated with treatment-related peripheral neuropathy. Older adults are at increased risk of falls compared to the general population, often leading to associated morbidity and mortality. While an association between peripheral neuropathy and falls in older adults is well-established, the relationship between bortezomib and falls in older multiple myeloma patients is unknown. Our primary aim was to determine if older patients with multiple myeloma treated with bortezomib as first-line therapy had an increased incidence of falls within the first 12 months after starting treatment. Our secondary aim was to assess the overall survival of patients who fell compared to those who did not among patients who lived more than 12 months after initiating treatment.
Methods: We analyzed the SEER-Medicare database for all patients 65 years old or older diagnosed with multiple myeloma between 2007 and 2013 and were enrolled in fee-for-service Medicare part A, B and D plans. The patients' corresponding Medicare claims data were analyzed through 2014 for myeloma treatments, fall claims, and covariates of interest. The primary outcome was accidental falls (E880-E888) occurring between 14 days to 12 months after starting multiple myeloma treatment. First-line therapy was defined as any anti-myeloma treatment administered within 14 days of starting multiple myeloma treatment, with bortezomib treatment being the focal independent variable. Cox regression was performed to determine the relative risk of having a fall after controlling for other covariates. Patients who started bortezomib after first-line therapy were censored at time of bortezomib commencement. The survival analysis included only patients who survived more than 12 months of starting treatment to allow landmark analysis of falls in the first year.
Results: Of 4,084 older adults with new multiple myeloma diagnoses undergoing first-line therapy, the median age was 75 (range 65-97) with 51% males. Bortezomib was used in first-line therapy for 2,052 (50%) patients, of which 157 (8%) patients experienced a fall within 12 months after starting treatment compared to 102 (5%) of patients not receiving bortezomib (p < 0.001). Bortezomib was associated with a 28% increase risk of falls (HR 1.29; 95% CI 1.00-1.65; p = 0.047).
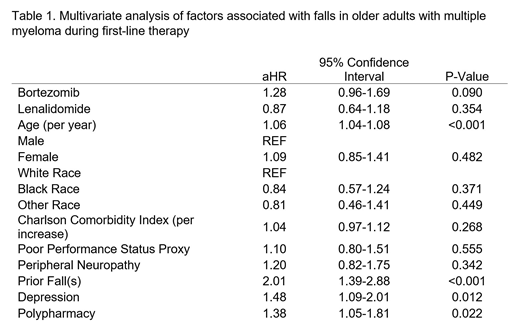
In multivariate analysis, bortezomib was not associated with an increased incidence of falls after controlling for age, gender, race, proxies for Charlson Comorbidity Index (CCI) and poor performance status, pre-existing peripheral neuropathy, falls within the 12 months prior to starting first-line myeloma treatment, depression, polypharmacy, and first-line treatment with lenalidomide (Table 1). Advancing age, history of fall(s), depression, and polypharmacy (defined as more than 10 unique prescription medications at initiation of first-line treatment), were all associated with an increased risk of falls, consistent with prior literature.
In a landmark analysis of those who survived 12 months following the start of treatment, a fall was associated with a 26% increased risk of hazard for death (aHR 1.26; 95% CI 1.02-1.56; p = 0.033) after controlling for other covariates. The median OS of those with a fall was 35.7 months (95% CI 29.1-48.4) compared to 49.1 months (95% CI 47.1-52.8) for those without (p < 0.0001).
Conclusion: In older adults with multiple myeloma, treatment with bortezomib was not associated with increased risk of a patient having a diagnostic code for falls. However, experiencing a fall within the year after starting treatment was associated with decreased overall survival. Limitations of the study include that the incidence of falls is likely underestimated in billing data, given prior data from our group showing a rate of self-reported falls of 26% in the year after diagnosis. Additional research, including prospective trials involving fall assessments, should be considered in older patients with multiple myeloma.
Wildes:Janssen: Research Funding; Carevive: Consultancy. Fiala:Incyte: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal