

Ruxolitinib (Rux), a potent JAK1/2 inhibitor, is the only FDA-approved drug for treatment of primary and secondary myelofibrosis (MF). Rux has been recently approved for treatment of steroid refractory acute graft-versus-host disease (GVHD), a major cause of non-relapse mortality (NRM) after allogeneic hematopoietic cell transplant (HCT). In MF patients proceeding with transplant, Rux is typically discontinued pre-HCT. Given the therapeutic, immunologic, and anti-inflammatory properties of Rux, we hypothesized that continuous peri-HCT administration of the drug is safe and can result in better transplant outcomes in MF patients. Here, we are reporting outcomes of our single arm, single center pilot study (NCT02917096) investigating the safety and efficacy of Rux administration in patients with primary or secondary MF undergoing HCT with fludarabine (125 mg/m2) and melphalan (140 mg/m2) as reduced intensity conditioning and sirolimus/tacrolimus (target levels: 5-10ng/ml for both) as GVHD prophylaxis. This pilot study is being conducted in MF patients with the goal of extending the therapy to other hematologic malignancies.
The primary objective was to identify the maximum tolerated dose and recommended phase II dose. Rux was given at 2 dose levels (DL) of 5 and 10 mg BID, starting from day -3 pre-HCT until day +30 post-HCT, then tapered off by day +33. DLs were chosen based on previous retrospective studies identifying the drug dose for treatment of GVHD. Primary endpoint was safety. Dose limiting toxicity (DLT) was defined as grade 4 neutropenia associated with fever, infection, or engraftment failure or any grade ≥3 non-hematologic toxicities over 45 days. Key secondary endpoints were grade 2-4 acute GVHD, engraftment, infection, overall survival (OS), progression-free survival (PFS), NRM, relapse and chronic GVHD.
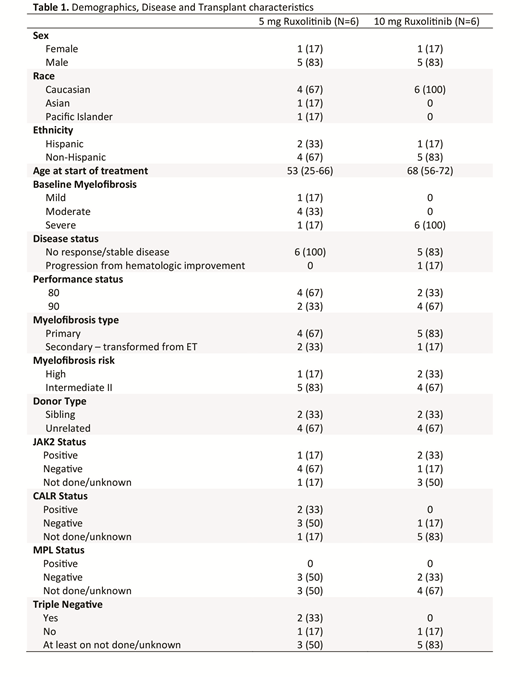
So far, we have enrolled 12 patients: 6 for DL1 arm and 6 for DL2. Median age at the time of HCT was 53 years (range: 25-66) for DL1 and 68 years (range: 56-72) for the DL2 arm. Detailed patient/transplant characteristics are listed in table 1. One-year OS, PFS and NRM for all patients were 80% (95%CI: 39-95), 68% (95%CI: 30-89) and 21% (95%CI: 3-50), respectively. All patients engrafted (n=12), with the median time to neutrophils engraftment of 19 days (range: 13-23) for DL1 and 16 days (range: 12-22) for the DL2 arm.
Hematologic DLTs were not observed in patients at either dose level. At DL1, by day +60, grade ≥3 toxicities were cardiac (n=1), pulmonary (n=1) and gastrointestinal (n=1). Only one case of grade ≥3 pulmonary toxicity was observed in patients at DL2. After median follow-up time of 373 days (range: 365-744) in DL1 and 98 days (range: 30-379) for DL2, there were two deaths; one due to respiratory failure in DL1, and another due to acute GVHD at DL2. Median time of acute GVHD onset was 20 days (range: 19-35) in DL1 and 51 days (range: 26-76) in DL2. Grade III-IV acute GVHD was seen in only 1 out of 12 patients and grade 1 acute GVHD was seen in 4 patients. One patient in DL1 relapsed at 9 months and re-entered remission with post-HCT treatment. CMV infection was seen in only 1 patient at DL2.
Pharmacokinetics (PK) studies were done for five patients at DL1 and all patients at DL2. PK was dose-proportional, in which doubling of the dose corresponded to the twice greater Cmax and AUC. The half-lives and oral clearances were not different between the two DLs. The Cmax and AUC were lower in our patients compared to a previously published report in healthy volunteers. Furthermore, the elimination half-life was similar to the published data, indicating that the lower drug exposures measured on the current trial is most likely due to decreased oral absorption. Lastly, GVHD biomarkers and inflammatory cytokines levels were not different between patients receiving Rux at DL1 and DL2.
In conclusion, early results of this pilot study indicate that Rux administration at 10 mg BID in MF patients undergoing HCT is safe and feasible, with 100% engraftment and low rate of acute GVHD. We are currently accruing an expansion cohort of 6 patients at DL2. Results of our PK studies indicated a direct correlation between Cmax and AUC and that higher oral clearance compared to previous study is most likely due to poor GI absorption of the drug in HCT patients. More follow up is needed to see the impact of this combination on incidence of chronic GVHD. This regimen may also be useful for patients undergoing HCT for other hematologic malignancies.
Palmer:Gilead Sciences: Consultancy. Salhotra:Celgene: Other: Research Support; Kadmon Corporation: Other: Non paid consultant. Mei:Seattle Genetics, Inc.: Research Funding. Nakamura:Celgene: Other: support for an academic seminar in a university in Japan; Alexion: Other: support to a lecture at a Japan Society of Transfusion/Cellular Therapy meeting ; Merck: Membership on an entity's Board of Directors or advisory committees; Kirin Kyowa: Other: support for an academic seminar in a university in Japan.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal