

Introduction:
Rituximab-based high-dose therapy (HDT) is frequently prescribed to DLBCL patients (pts) undergoing auto-HCT. However data supporting the benefit of adding R to auto-HCT conditioning are not available. Herein, we report the impact of R-based conditioning on auto-HCT outcomes of DLBCL pts.
Methods:
Using the Center for International Blood and Marrow Transplant Research registry, 862 adult (≥18 years) DLBCL pts undergoing auto-HCT, between 2003-2017 were included. Analysis was limited to pts receiving BEAM (BCNU, etoposide, cytarabine, melphalan)-based HDT, as R was infrequently used with non-BEAM conditioning regimens. All pts received R-containing chemoimmunotherapy in the frontline setting and had chemosensitive disease prior to HCT. Early chemoimmunotherapy failure (ECitF) was defined as not achieving a complete remission (CR) after frontline chemoimmunotherapy or relapsing within 1 year of initial diagnosis. Primary outcome was overall survival (OS). Secondary outcomes included non-relapse mortality (NRM), relapse, progression-free survival (PFS) and infectious complications within 100 days post-HCT.
Results:
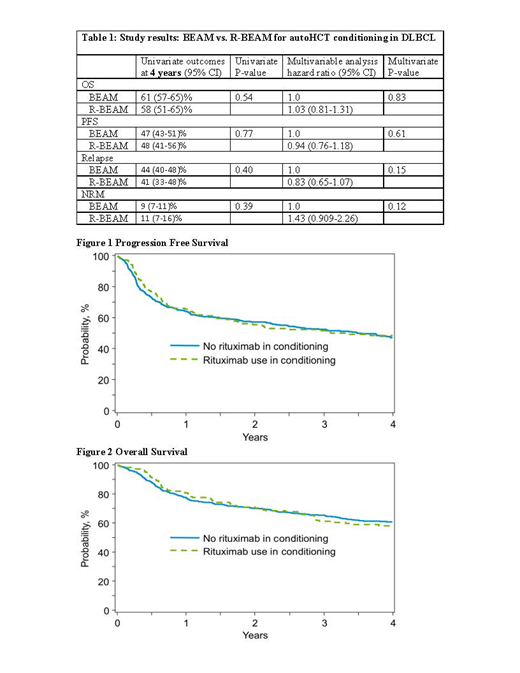
The study cohort was divided into 2 groups; BEAM (n=667) and R-BEAM (n=195). The baseline characteristics of the 2 cohorts were comparable including age at auto-HCT, disease stage, Karnofsky performance score, extranodal involvement, time from diagnosis to auto-HCT, number of prior therapies, remission status, and ECitF. However, significantly more R-BEAM cohort patients received R as part of last therapy line before auto-HCT (75% vs. 86%; P=0.001). Median follow-up of survivors was 48 (range 1-171) and 64 (range 3-142) months in the BEAM and R-BEAM cohorts, respectively. On univariate analysis, the 4 year cumulative incidence of relapse (41% vs 44%), NRM (11% vs 9%), PFS (48% vs 47%; Figure 1) and OS (58% vs 61%; Figure 2) were similar in the R-BEAM and BEAM groups, respectively (Table 1). On multivariate analysis, no significant difference was seen in OS (HR 0.81; 95% CI 0.81-1.31; P=0.83) or PFS (HR 0.94; 95% CI 0.76-1.18; P=0.61) (Table 1) between the two cohorts. Addition of R had no impact on risk of relapse (HR 0.83; 95% CI 0.65-1.07; P=0.15) or NRM (HR 1.43; 95% CI 0.909-2.26; P=0.12). Variables independently associated with lower OS included older age (HR 3.05; 95% CI 1.81-5.13; P<0.001), not being in CR at auto-HCT (HR 1.67, 95% CI 1.39-2.07; P<0.001) and presence of ECitF (HR 1.52, 95% CI 0.54-3.26; P<0.001). Older age (HR 2.26, 95% CI 1.48-3.45; P<0.0002) and not being in CR at auto-HCT (HR 1.78, CI 1.47-2.14; P<0.0001) were also associated with inferior PFS. There was no significant difference in the 100-day cumulative incidence of bacterial, viral or fungal infections between the two cohorts. Disease relapse was the main cause of death in both BEAM and R-BEAM cohorts (66% vs 55%).
Conclusion:
In this large registry analysis of DLBCL pts undergoing auto-HCT, adding R to BEAM conditioning had no impact on transplantation outcomes. Older age, absence of CR and ECitF were associated with inferior survival.
Majhail:Mallinckrodt: Honoraria; Incyte: Consultancy; Nkarta: Consultancy; Anthem, Inc.: Consultancy; Atara Bio: Consultancy. Sureda:Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel Support; Gilead: Honoraria; Amgen: Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Honoraria, Speakers Bureau; Novartis: Honoraria; BMS: Honoraria; Roche: Honoraria; Sanofi: Honoraria; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees. Kharfan-Dabaja:Daiichi Sankyo: Consultancy; Pharmacyclics: Consultancy. Hamadani:ADC Therapeutics: Consultancy, Research Funding; Merck: Research Funding; Takeda: Research Funding; Pharmacyclics: Consultancy; Celgene: Consultancy; Medimmune: Consultancy, Research Funding; Janssen: Consultancy; Otsuka: Research Funding; Sanofi Genzyme: Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal